Download
1 / 41
1.51k likes | 5.91k Views
Child with anemia. Marie-Claude laplante. Objectives. To develop an approach to the child with anemia To identify clinical manifestations of severe anemia To determine the appropriate laboratory investigations in a child with anemia

E N D
Child with anemia Marie-Claude laplante
Objectives To develop an approach to the child with anemia To identify clinical manifestations of severe anemia To determine the appropriate laboratory investigations in a child with anemia To review the laboratory and clinical features of hemoglobinopathy and transient erythroblastopenia of childhood To determine the short and long term management of iron deficiency
Case 18 month old boy Italian descent seen for routine immunization History reveals that the child is well with no parental concerns other than their relatives have recently mentioned that the child is pale looking. He did have a viral URTI last week. You seek a dietary history and parents state that the child is a very picky eater. He eats pasta and chicken only. He also drinks six eight ounce bottles of homogenized milk daily. They have also noticed lately that he is eating the stuffing from his toy animals and is chewing on carpeting.
Case (2) • On physical examination you observe a chubby, pale child. Vital signs are: • HR: 140/min • RR: 24/min • BP: 90/60 • Weight is slightly above the 95th percentile for age, and his height is the 50th percentile for age. He is quietly playing. Auscultation reveals equal air entry bilaterally with no crakles. • There is a systolic ejection murmur at the left sternal border graded II/IV. There is no hepatosplenomegaly and no lymphadenopathy. The hands and feet are puffy
Case (3) • Blood work: • CBC: • Hemoglobin 43g/L • WBC 8.2 x 109 /L with a normal differential • Platelet count 765 x 109 /L • MCV 56fL • Reticulocyte count: 20 • Peripheral blood smear: 4+ hypochromic/microcytic red cells
Basic physiology Stimulus:
Basic physiology Adult: • Hb A (a2 b2) 96 - 98 % • Hb A2 (a2d2) 1,5 - 3,0 % • Hb F (a2g2) 0,5 - 1,0 %
Basic physiology • Erythropoeisis: • Fetal: • 4-5 weeks: Primitive megaloblasticerythropoiesis in yolk sac • 6 weeks: Transition to normoblasticerythropoiesis in the liver. • 3 months: Haematopoiesis begins in spleen, thymus and lymph nodes (principle organ remains liver) • 4 months: Bone marrow haematopoiesis begins and increases with gestation. • Birth: • Birth – 1 week postnatal: Liver and spleen continue haematopoiesis • Bone marrow volume expands
Basic physiology • Erythropoesis: • Newborn: • Decreases dramatically in first week as oxygen is readily available for tissues (physiologic anemia of infancy)
General approach to anemia • Definition: • Anemia may be defined as a reduction in red blood cell (RBC) mass or blood hemoglobin concentration. In practice, anemia most commonly is defined by reductions in one or both of the following: • Hematocrit (HCT) — The hematocrit is the fractional volume of a whole blood sample occupied by red blood cells (RBCs), expressed as a percentage. As an example, the normal HCT in a child age 6 to 12 years is approximately 40 percent. • Hemoglobin (HGB) — This is a measure of the concentration of the RBC pigment hemoglobin in whole blood, expressed as grams per 100 mL (dL) of whole blood. The normal value for HGB in a child age 6 to 12 years is approximately 13.5 g/dL (135 g/L). ** In pediatrics, anemia is defined as a hemoglobin level of less than the 5th percentile for age or 2 SD below mean value for age.
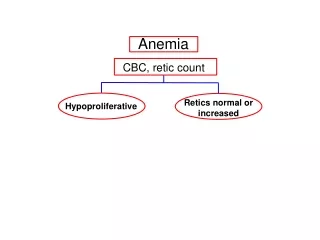
General approach to anemia Recognizing clinical features (signs and symptoms) Recognizing the need for screening patients otherwise asymptomatic at high risk Ordering the right laboratory tests Analyzing the data and narrowing the differential Treating/ordering additional testing to narrow the differential further
General approach to anemia • Screening: • Not recommended unless child is at risk: • Prematurity • Poor diet • Consumption of more than 24oz of cow’s milk per day • Chronic blood loss or illness • Drug use • Ethnicity : • Africans, Mediterranean and Asians in thalassemia • Sephardic Jewish, Filipino, Greek, Sardinian or Kurdish ancestry in G6PD deficiency • Family history • Mechanical heart valves • Sex (more common in males) • Splenomegaly • Infection
History *Most children are asymptomatic! • Typical pediatric history: • HPI • Maternal history (pregnancy/delivery complications, drugs, pica, anemia) • Family history (ethnicity!) • Patient history including: • Palpitations • Shortness of breath • Pica • Irritability/inappropriate behaviour • Jaundice • Low activity level/sleepiness/tiredness • Evidence of chronic infection/disease, liver disease or endocrinopathy • Medications • Diet history (*emphasis on cow’s milk consumption) • Easy bruising/blood loss (stool pattern, hematochezia)
Physical • You may find: • Tachycardia • Tachypnea • Pallor of conjunctivae, tongue, palm or nail bead • Petechiae (multiple cell lineages involved) • Tortuosity and narrowing of fundal vessels/cork screw vasculature of conjunctiva • Decreased vibration and position senses • Splenomegaly • Jaundice • Heart failure (severe acute anemia) • Glossitis, flow murmur and growth delay may be seen in severe chronic disease
Investigations – initial evaluation • CBC • White blood cell count (+/- differential) • Differential: neutrophils, lymphocytes, monocytes, eosinophils, basophils and immature neutrophils called bands) • Red blood cell count • Hematocrit • Hemoglobin • Red blood cell indices • Mean corpuscular volume, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, red cell distribution width. • Platelet count • Mean platelet volume • Peripheral blood smear
Approach to childhood anemia - Newborn • Major causes: • Blood loss • Ruptured cord, placenta previa, placental abruption • *Use of forceps and vacuum in delivery can cause cranial hemorrhages, especially subgaleal bleeds (between periosteum and scalp) • Decreased RBC production (marrow): • Fanconi anemia, Diamond Blackfan syndrome and congenital infections (B19, HIV, syphilis, rubella, sepsis) • Increased RBC turnover/destruction: • Isoimmunization: ABO or Rh incompatibility • Congenital hemolytic (spherocytosis, G6PD deficiency)
Approach to childhood anemia – Infant to toddlerhood Iron deficiency Concurrent infection Blood loss (trauma, GI) Disorder of Hgb structure or synthesis (thalassemia, sickle cell) RBC enzyme defects (G6PD deficiency, pyruvatekinase deficiency) RBC membrane defects (spherocytosis, elliptocytosis) Acquired hemolytic anemias (drug, antibody, DICS) Transient erythroblastopenia of childhood Leukemia, myelofibrosis Lead poisoning
Transient erythroblastopenia of childhood • Definition: • Subtype of pure red cell aplasia which refers to a type of anemia affecting the precursors to red blood cells, but not to white blood cells. • Transient immune reaction against erythroid progenitor cells. • Epidemiology: • Most common cause of decreased RBC production in children. • M>F • Etiology: • Unknown, possible causes include viral illness, cell-mediated supression, genetic predisposition…
Transient erythroblastopenia of childhood • Clinical findings: • Usually seen in patients 6 months – 3 years of age • Typically, these patients are clinically NORMAL, but we may see a gradual onset of pallor. • Hematologic findings: • Normocytic anemia • Reticulocytopenia • Mild neutropenia in over 50% of patients • Platelets normal-elevated • Treatment: • Clinical course of ~2 months, most patients present in recovery • Red blood cell transfusions may be considered when severe cardiorespiratory symptoms or fatigue that interferes with quality of life are present.
Hemoglobinopathy • 3 potential issues: • Abnormal structure of hemoglobin (Hb SS, Hb C, Hb D, Hb E etc.) • Qualitative issue • Abnormal production of hemoglobin (thalassemia) • Quantitative issue • Mixed
Sickle cell disease • Pathophysiology: http://www.youtube.com/watch?v=R4-c3hUhhyc • Clinical features: • Acute painful crises: • First symptom of disease in >25% of cases • Peaks at ages 19-39 • Intensity and frequency of painful episodes varies considerably • May be precipitated by weather, stress, dehydration, infection, mensies, alcohol, OSA, etc. • Multiorgan failure syndrome is most often seen during crises, but the pathophysiology remains uncertain.
Sickle cell disease • Clinical features: • Psychosocial issues • Growth and development (common growth failure and delayed puberty) • Reduced or absent splenic function (due to multiple infarcts) • Infection susceptibility (secondary to splenic function) • Cerebrovascular events (24% experience stroke before age 45) • Bone complications (osteonecrosis and infarction) • Cardiac complications (infarction) • Dermatologic complications (leg ulcers) • Hepatobiliary complications • Priapism • Pulmonary complications • Renal complications • Retinopathy
Sickle cell disease • Investigations: • CBC: • Mild-moderateanemia: • Hematocrit 20-30% • Reticulocytosis 3-15% • Leukocytosis • Thrombocytosis (splenicdysfunction) • PBS: • RBC usuallynormocytic and normochromic • Howell-Jolly bodies (reflecthyposplenia) • Sickledredcells • Polychromasia (reticulocytosis) • Hemoglobinelectrophoresis
Thalassemia • 2 types: • α-thalassemia : lowsynthesis or absence of α chains • β-thalassemia : lowsynthesis or absence of β chains
Thalassemia – Alpha • Clinical features: • 1 gene defect: silent carrier, asymptomatic • 2 gene defect: • Cis type = minor anemia, usually asymptomatic • Trans type = minor anemia, usually asymptomatic • 3 gene defect: H disease, severe anemia • 4 gene defect: Bart’s hemoglobin = hydropsfetalis and fetal or neonatal loss • Investigations: • HgB and HCT usually within normal range • Typically marked microcytosis and hypochromia • Electrophoresis: no increase in HgB-A2
Thalassemia – Beta • Clinical features: • Low HgB-A therefore: • Pallor is most common • Other signs/symptoms as seen previously • Failure to respond to therapy for presumptive iron deficiency anemia • Investigations: • Typically microcytic and hypochromic • Basophilic stippling can be observed with a Wright stain • Mentzer index: MCV/red cell count per milliliter <13 • *Higher than 13 in iron deficiency • Electrophoresis: presence of high HgB-A2, HgB-F or HgB-E
Iron deficiency • Why is it so important?? • Most common nutritional deficiency in children – WHO estimates it affects 25% of the world’s population (concentrated within children and women). • 9% of toddlers in the United States, 2-3% have resulting anemia
Iron deficiency • Signs and symptoms: • Mostly asymptomatic, often pallor is the only sign • Patients with mdoerate-severe anemia: • Lethargy/poor feeding • Pallor • Irritability • Cardiomegaly • Tachypnea • Neurodevelopmental (impaired psychomotor and/or mental development) • *Occasionally PICA and pagophagia
Iron deficiency - Management • Microcytic <24 months (mild symptoms): • Often caused by iron deficiency, therefore you can treat presumptively with oral iron therapy and repeat testing in 1 month. • 3-6mg/kg of elemental iron per day (typically ferrous sulfate) • Max 150mg daily • Counsel on feeding whole cow’s milk • Associated with protein-induced colitis – intestinal blood loss • Continue treatment for 2 months after the normalization of Hgb • If there’s no response after 1 month, consider other causes: • CBC, FOBT, PBS, FOBT, lead testing, B12/folate levels, Hgb electrophoresis
Iron deficiency - Management • Microcytic >24 months (mild symptoms) • Iron deficiency less common • Initial investigations should include: • CBC, reticulocytes, PBS and FOBT • If PBS is hypochromicmicrocytic and there’s no evidence of GI loss or lead toxicity, treat with iron at same dosage.
Iron deficiency - Management • In severe cases (Hgb<7): • Initial investigations should include: • Ferritin, serum iron, TIBC and transferring saturation • FOBT • Possible treatment options include: • Parenteral iron therapy: • Severe persistant anemia with proven intolerance to supplements, malabsorption or poor compliance. • Iron dextran is most commonly used • Blood transfusion: • Rarely necessary • To be reserved for patients in distress (HR>160bpm, RR>30, lethargy, not feeding well) • 5mL/kg over 3-4 hours
Approach to anemia – Late childhood and adolescence Iron deficiency Chronic disease Blood loss Disorders of Hgb synthesis or RBC membrane defects Acquired hemolytic anemias Leukemia and other marrow disorders
Back to the case! • 18 month old boy • Italian descent • Child is well, no parental concerns • Relatives mentioned that the child is pale looking. • Viral URTI last week. • Diet: • Very picky eater; pasta and chicken only. • Drinks six eight ounce bottles of homogenized milk daily (48oz/24hrs) • They have also noticed lately that he is eating the stuffing from his toy animals and is chewing on carpeting.
Case (2) • On physical examination you observe a chubby, pale child. Vital signs are: • HR: 140/min • RR: 24/min • BP: 90/60 • High weight, normal height • Weight 95th percentile for age, height 50th percentile for age. • There is a systolic ejection murmur at the left sternal border graded II/IV. • There is no hepatosplenomegaly and no lymphadenopathy. • The hands and feet are puffy.
Case (3) • Blood work: • CBC: • Hemoglobin 43g/L • WBC 8.2 x 109 /L with a normal differential • Platelet count 765 x 109 /L • MCV 56fL • Reticulocyte count: 20 • Peripheral blood smear: 4+ hypochromic/microcytic red cells
References Finne, H. & Halvorsen, S. (1972) Regulation of Erythropoiesis in the Fetus and Newborn, Disease in Childhood, 47, p. 683-87. Hermiston, M., Mentzer, W. (2002) A practical approach to the evaluation of the anemic child, The Pediatric Clinics of North America, 49, p.877-91. Janus, J. & Moerschel, S. (2010) Evaluation of Anemia in Children, American Family Physician, 81(12), p.1462-71. Marieb, E.N. (2005). Le sang, In Anatomie et physiologiehumaines (3rd ed., p. 663-695). Pearson Education Inc. Richardson, M. (2013) Microcytic Anemia, Pediatrics in Review, 28(5), p.5-14. Segel, G. (1988) Anemia, Pediatrics in Review, 10(3), p. 77-88. Segel, G., Hirsh & M., Feig, S. (2002) Managing Anemia in Pediatric Office Practice Part 1, Pediatrics in Review, 23(3), p. 75-84. Uptodate