Download
1 / 19
200 likes | 351 Views
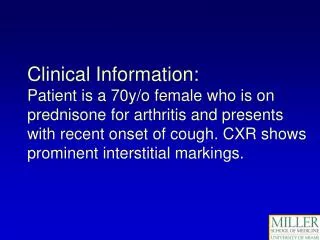
Improving the Patient Experience: H-CAHPS. Quality Improvement Project Invasive/Non Invasive Cardiology. Membership. Cardiology Quality Council Theresa Fortner -Nurse Manager Invasive Cardiology Joelyn Niggel - Nurse Manager NI Cardiology Karen McKenny - Nurse Educator

E N D
Improving the Patient Experience: H-CAHPS Quality Improvement Project Invasive/Non Invasive Cardiology
Membership • Cardiology Quality Council • Theresa Fortner -Nurse Manager Invasive Cardiology • Joelyn Niggel - Nurse Manager NI Cardiology • Karen McKenny - Nurse Educator • Julie Eastman - RN Invasive Cardiology • Kristin Pelkey - Cardiology Tech NI Cardiology • Kathy Getty - RN Invasive Cardiology • Judy Rent - RN Invasive Cardiology • Heidi Igneri - RN Invasive Cardiology • Melissa Lambert - Supervisor Cardiology Tech Dept. • Mike Socha - Supervisor Cardiac Ultrasound • Karen McKnight - Quality Consultant
Hospital Consumer Assessmentof Healthcare Providers& Systems The survey and data collection methodology are mandated by the government. The survey, methodology and results are in the public domain. H-CAHPS is publicly reported on: www.hospitalcompare.hhs.gov www.hcahpsonline.org What is the H-CAHPS Survey
Background • Goals: H-CAPHS • Compare hospital perspective and patient perspective • Ensure the highest quality of patient care and understanding • History: • 2006 Voluntary collection began • 2008 FAHC first participated • 2010 Government regulated • 2011 Value based purchasing rule finalized
Background • Not a satisfaction survey • Measures the behaviors of staff from the patients perspective • Patient Mix Adjusted (age, health, medicine, surgery, OBS) • Not limited to Medicare patients • Nursing and Physician based questions
Background • Reimbursement • Government will hold 1% of Medicare payments • FAHC can earn back the 1% if we meet National Bench Mark Performance • Reimbursement is based on a % • This is expected to increase to 2% by 2017
Objectives • Educate the staffregarding H-CAPHS • Develop a Cardiology Code of Conduct for improving patient experience. • Improve the patient experiencein procedural areas. • Distribute Thank You cards to allinvasiveoutpatients post procedure
Methodology • Education of Staff: • Presentations by content experts • Staff meetings in all departmentsaddressing H-CAHPS and concerns regarding: communication, privacy, noise, and environment • Email • Cardiology Quality Council to develop a Cardiology Code of Conduct based on staff feedback • Redesign the current AIDET survey tool to meet the needs of a procedural area. • Monthly auditing of all procedural areas • Review results: H-CAHPS and Press Ganey Surveys
Implementation • Cardiology Code of Conduct • Staff Education • Monthly Audits • Thank You Note
Cardiology Code of ConductWays to impact the patient experience in a positive manner • Communication: Cardiology Staff/Providers/Fellows • Communicate with patient and patient’s family of delays. Use “blameless apology” • Show concern for patient verbally as well as nonverbally • Introductions • Shows patient respect, courtesy, and confidence • Delays and updates • Privacy • Maintain the patient’s physical privacy in the testing areas at all times.
Cardiology Code of Conduct • Noise • In testing areas- pre and post procedure. • Music • Television • Staff • Schedulers • Vendors • Monitor control room • Physician pagers during procedures • Environment • Environmental Services
Action Plan/Next Steps • Further revision of the AIDET tool • Forming it to fit the needs of the testing area • Clarifying aspects of AIDET • Continued education for staff • Education of auditing staff • How to use tool • Inter-rater reliability • Continued monthly auditing • Thank you cards: • Roll out to Non Invasive testing areas in 2012
H-CAHPS CARDIOLOGY Displayed by Discharged Date
SEPTEMBER Cardiology M5 AUGUST August September