Download
1 / 72
730 likes | 770 Views
Hyperhidrosis. Dr Abbas Pardakhty 2011 Kerman Faculty of Pharmacy. Sweat Glands. The human body has 2-5 million sweat glands Two main types:. ECCRINE. APOCRINE. Source: www.sweathelp.org. Eccrine Sweat Glands. Approximately 3 million eccrine sweat glands Secrete a clear, odorless fluid

E N D
Hyperhidrosis Dr Abbas Pardakhty 2011 Kerman Faculty of Pharmacy
Sweat Glands • The human body has 2-5 million sweat glands • Two main types: ECCRINE APOCRINE Source: www.sweathelp.org
Eccrine Sweat Glands • Approximately 3 million eccrine sweat glands • Secrete a clear, odorless fluid • Aid in regulating body temperature • Areas of concentration: • Facial, plantar, and axillae Source: www.sweathelp.org
Apocrine Sweat Glands • Inactive until puberty • Produce thick fluid • Secretions come in contact with bacteria on the skin and produce characteristic “body odor” • Found in axillary and genital areas Source: www.sweathelp.org
Sweating • The hypothalamus serves as the thermoregulatory center • It controls both blood flow and sweat output to the skin’s surface Source: www.sweathelp.org
Sweating • The hypothalamus can be triggered by: EXERCISE STRESS TEMPERATURE CHANGE HORMONES Source: www.sweathelp.org
Sweating Once triggered, the hypothalamus sends messages down the spinal cord via neurotransmitters. Source: www.sweathelp.org
Sweating The neurostransmitters travel down the spine via ganglion or sympathetic nerves These ganglion travel to nerves, which reach the skin’s surface Source: www.sweathelp.org Photo used with permission: The Whiteley Clinic,2007
Neurotransmitters Neurotransmitters act as “vehicles,” transmitting information from the hypothalamus to the skin’s surface. Photo used with permission: The Whiteley Clinic, 2007
Neurotransmitters The neurotransmitters can “exit” at various places along the spinal cord. The “exit” determines the location of skin innervation.
Spinal Cord Innervations T2-T4 innervate the skin of the face T2 – T8 innervate the skin of the upper limbs T4-T12 innervate the skin of the trunk T10-T12 innervate the skin of the lower limbs Source: www.sweathelp.org
Neurotransmitters Acetylcholine innervates Catecholamines innervate Eccrine Sweat Glands Apocrine Sweat Glands Source: www.sweathelp.org
Sweating Once innervated, the apocrine and eccrine glands will produce …. SWEAT! Source: www.sweathelp.org
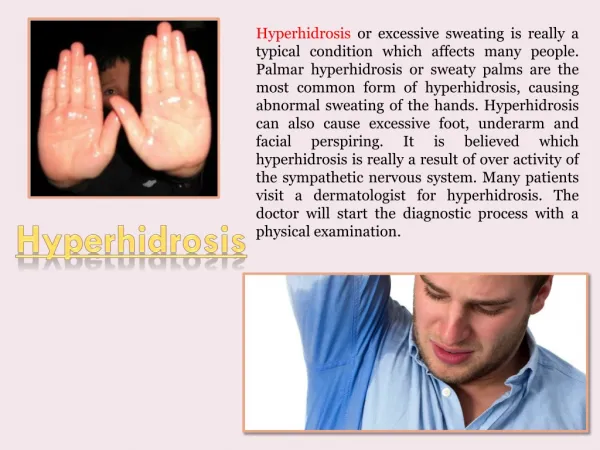
What is Hyperhidrosis? • Sweating that is more than required to maintain normal thermal regulation
Sweating Nomenclature • Areas: Focal, regional, generalized • Symmetry: Symmetric or asymmetric • Classification: Primary vs. secondary • Type of sweating: Anhidrosis, euhydrosis, hyperhidrosis Multi-specialty Working Group on Recognition, Diagnosis, and Treatment of Primary Focal Hyperhidrosis, 2003.
Causes of Generalized Hyperhidrosis Usually secondary in nature • Drugs (Venlafaxine, ...), toxins, substance abuse • Cardiovascular disorders • Respiratory failure • Infections • Malignancies • Hodgkin’s, myleoproliferative disorders, cancers with increased catabolism • Endocrine/metabolic disorders • Thyrotoxicosis, pheochromocytoma, acromegaly, carcinoid tumor, hypoglycemia, menopause • Rarely Idiopathic / Primary HH
Causes of Localized Hyperhidrosis • Usually Idiopathic / Primary • Social anxiety disorder • Eccrine nevus • Gustatory sweating • Frey syndrome • Impaired evaporation • Stump hyperhidrosis after amputation
Diagnosis of Primary Focal Hyperhidrosis • Focal, visible, excessive sweating of at least 6 months duration without apparent cause with at least 2 of the following characteristics: • Bilateral and relatively symmetric • Impairs daily activities • Frequency of at least one episode per week • Age of onset less than 25 years • Positive family history • Cessation of focal sweating during sleep Multi-specialty Working Group on Recognition, Diagnosis, and Treatment of Primary Focal Hyperhidrosis, 2003.
Diagnostic Work-up • History • Age of onset • Location • Trigger factors • Review of symptoms • Physical exam • Laboratory evaluation • Gravimetric – 1° research tool • Starch iodine – defines area of disease Starch iodine test, with the darkened area showing location of excessive sweating
Axillary Sweat Production 346.0 1° hyperhidrosis patients healthy controls Hund et al. Arch Derm 2002;138(4):539-41
DLQI Total Scores and Ranges by Dermatological Disease/ConditionDiseases with DLQI Scores 10 or Greater Disease DLQI Score (baseline) Hyperhidrosis palms 18–8.8 Hyperhidrosis axillary 17–10 Eczema (inpatient) 16.2 Focal hyperhidrosis (general) 15.5–9.2 Psoriasis (inpatient) 13.9 Hyperhidrosis forehead 12.5 Atopic eczema 12.5–5.8 Psoriasis (outpatient) 11.9–4.51 Contact dermatitis 10.8 Pruritus 10.5–10 Scores range from 0 to 30, with 30 indicating the worst quality of life. Spalding et al. Value in Health 2003;6(3):242(abstract)
Summary Primary Focal Hyperhidrosis is a separate and unique disease • Bilateral & symmetric • Axilla, palms, soles, craniofacial • Onset in childhood and adolescence • Significant impact on quality of life • Effective therapies
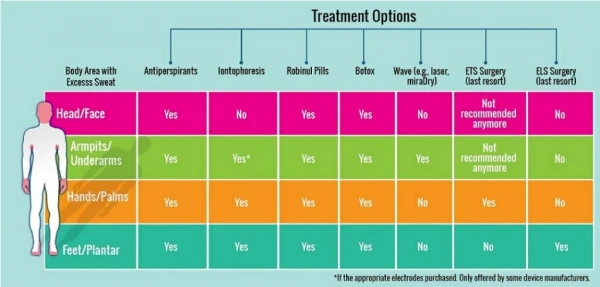
Available Treatments • Topical agents • Iontopheresis • Systemic agents • anticholnergic • Botulinum toxin • Surgery • Local excision/currettage • Thoracic sympathectomy
Treatment Options Topical Click on the first treatment option to begin! Systemic Iontophoresis Botox Local Excision Thorascopic Sympathectomy
Topical Treatment • First line treatment • Aluminum Chloride Hexahydrate • antiperspirant of choice • Most beneficial for axillary hyperhidrosis • Can be used for plantar and palmar Photos used with permission: www.feelbest.com Hornberger, 2004
Topical Treatment:How Does it Work? The metal ions in the topical antiperspirant damage the lining of the sweat gland. As damage continues, a PLUG is formed over the sweat gland. www.sweathelp.org
Topical Treatment • Sweat production never ceases, the gland is simply plugged • Sweating will return as the skin undergoes regeneration or shedding • Therefore…topical treatment is NOT a cure! Photo used with permission: Neurosurgical Medical Clinic, Inc Hornberger, 2004
Topical Treatment:How to Use • Best to apply before bedtime • Allow to remain on skin for 6 – 8 hours • Apply every 24 – 48 hours until sweating diminishes • Maintenance applications needed every 1-3 weeks Hornberger, 2004
Topical Treatment: Pros and Cons Non – invasive Itching and burning of skin at application site & Time-consuming & Temporary relief Hornberger, 2004
Topical Treatment:Effectiveness 88% effective for Axillary Hyperhidrosis 66.6% stop using due to the “CONS” Naumann, Hamm, & Lowe, 2002
Treatment Options Topical Click on the second treatment option! Systemic Iontophoresis Botox Local Excision Thorascopic Sympathectomy
Systemic Treatment • Anticholinergics can be used in treating hyperhidrosis • Most effective for cranio-facial hyerhidrosis • Robinul – drug of choice Haider & Solish, 2004
How Does it Work? Anticholinergic Blocks Acetylcholine transmission Eccrine sweat glands no longer stimulated Sweat production ceases! Haider & Solish, 2004
Anticholinergics • Long term therapy is required • Major side effects: • Dry mouth • Dry eyes • Constipation • Blurred vision • Difficulty with urination Thomas, Brown, & Vafaie, 2004
Anticholinergics • Limited use in treating hyperhidrosis • Only 21% effective • 69.7% stop using due to side effects Hamm, Naumann, & Kowalski, 2006
Topical anticholinergics • glycopyrronium bromide as 1 and 2% cream or roll-on solution • Topical hyoscine as 0.25, 1, or 3% solution or cream also gave control of sweating, but was associated with a much higher incidence of side-effects. • Patients with diabetic gustatory sweating have also noted a reduction in the frequency and severity of episodes after applying glycopyrronium 0.5% cream
Treatment Options Topical Click on the third treatment option! Systemic Iontophoresis Botox Local Excision Thorascopic Sympathectomy
Iontophoresis • Used for palmar and plantar hyperhidrosis • Passage of direct electrical current onto skin’s surface • Device can be purchased for home use Photo used with permission: Beast Psoriasis, 2006 Thomas, Brown, & Vafaie, 200 4
Iontophoresis • Sit with hands or feet in shallow tray of water • Allow 15 – 20 milli-amps of electrical current to pass through water • Use for 10 days, 30 minutes each day • Maintenance therapy needed Photo used with permission: Beat Psoriasis, 2006 Thomas, Brown, & Vafaie, 2004
Iontophoresis:Mechanism of Action Thickening of skin And Blocked sweat flow + = ELECTRICTY WATER www.sweathelp.org
Iontophoresis • Side effects: • Skin irritation • Skin burns • Vesicle formation • Time consuming treatment • 80% effective for palmar and/or plantar hyperidrosis Photo used with permission: Beat Psoriasis, 2006 Thomas, Brown, and Vafaie, 2004
Treatment Options Topical Click on the fourth treatment option! Systemic Iontophoresis Botox Local Excision Thorascopic Sympathectomy