Download

1 / 60
600 likes | 621 Views
Explore the classification, mechanisms, and management of Na channel blockers toxicity. Learn about Class 1 anti-dysrhythmics, TCA's, propoxyphene, SSRI’s, neuroleptics, and more. Understand EKG findings and different antidysrhythmic drugs.

E N D
Toxicology 6:Na Channel Blockers Thanks to: P. Ukrainetz S. McPherson
Outline • Na Channel Blockers • Class 1 anti-dysrhythmics • TCA’s • Propoxyphene • Other Pharmacology • SSRI’s • Neuroleptics
What we won’t cover • Cocaine • Local anesthetics • Pufferfish
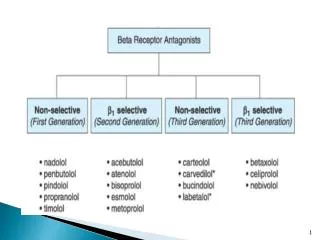
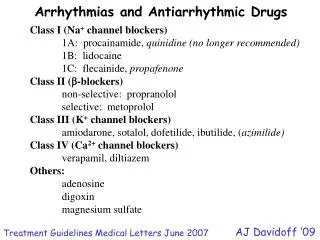
Antidysrhythmics • Classification: • Class 1: Na Channel Blockers • Class 2: Beta Blockers • Class 3: K Channel Blockers • Class 4: Ca Channel Blockers • Class 5: Other
The Sodium Channel • Voltage gated • 3 phases • Slow and fast
Increased automaticity Triggered activity Re-entry with unidirectional block Tachyarrhythmias
Anti-dysrhythmics Board Work
DDx wide qrs Class 1a Class 1c Cyclic anti-depressants Propoxyphene Cocaine Local anesthetics
Procainamide Disopyramide Quinidine Class 1a
Procainamide • IV, IM, or PO • Renally excreted • 1/3 lupus-like syndrome
Procainamide • NAPA • ACLS: indications? • Dosing?
Manamement of OD • ABC’s, monitor • EKG • HCO3 if wide qrs* • Consider Ca, glucagon • Lidocaine for dysrhythmias • TdP: Mg, pacing • AVOID: 1c/1a, BB, CCB
Lidocaine Tocainide Mexiletine Phenytoin Class 1b
Lidocaine • CNS, cardiac, and GI toxicity • Usually mild, dose-dependant • Low pro-arrhythmia risk? • ACLS: Indications? Dosing?
Management • Basic resuscitation as in Ia • “Non-responsive” bradycardia’s • Charcoal
Flecainide Propafenone Class 1c
Flecainide • Oral, IV • PR/QRS without QT • Increase mortality in cardiac pt’s • Primary use: outpt. afib
Management • Basic resuscitation • HCO3 • Amiodarone • Avoid other 1a/1c
Pt. called 9-1-1 after overdose Empty bottle of TCA on scene Normal strip. Stable TCA’s
TCA’s By what mechanisms do TCA’s exert their effects?
Mechanisms • Na channel blockade • K channel blockade • Gaba antagonism • Amine re-uptake inhibitor • Anticholinergic • Alpha-blocker
Bottom Line: Unpredictable
IV, O2, Monitor Vitals Case continued
EKG • Three benefits: • Diagnosis • Prognosis • Effect of treatment
Prognosis and EKG • QRS duration • Terminal 40ms • aVR findings
Bottom Line • Useful to consider these measurements -not 100% sensitive -useful if absent (to confirm lack of cardiac toxicity) -serial ECGs -do not use in isolation
Bottom Line: Does not correlate with toxicity Does not predict complications
Management? Case Continued
“Nearly all cases” PHAILS 1mg/kg Consider MDAC Charcoal?
Life-threatening Non-absorbable No antidote Early Gastric Lavage
Potentially toxic SR preparation Non-absorbable and no other method of decontamination Removal of Packets Whole Bowel Irrigation
NOT EFFECTIVE Elimination Urinary Alkalinization Dialysis
HCO3 - • Mainstay of therapy • 1-2meq/kg • Q3-5 min boluses • +/- infusion