Download
1 / 7
70 likes | 212 Views
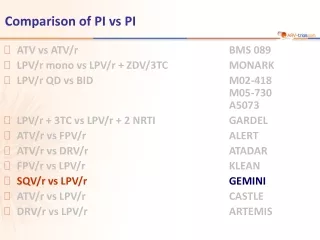
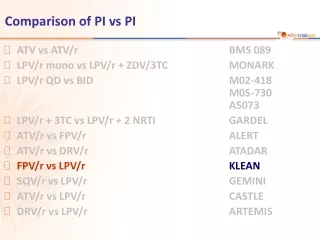
Comparison of PI vs PI. ATV vs ATV/r BMS 089 LPV/r mono vs LPV/r + ZDV/3TC MONARK LPV/r QD vs BID M02-418 M05-730 A5073 ATV/r vs FPV/r ALERT FPV/r vs LPV/r KLEAN SQV/r vs LPV/r GEMINI ATV/r vs LPV/r CASTLE DRV/r vs LPV/r ARTEMIS. KLEAN.

E N D
Comparison of PI vs PI • ATV vs ATV/r BMS 089 • LPV/r mono vs LPV/r + ZDV/3TC MONARK • LPV/r QD vs BIDM02-418M05-730A5073 • ATV/r vs FPV/r ALERT • FPV/r vs LPV/rKLEAN • SQV/r vs LPV/r GEMINI • ATV/r vs LPV/r CASTLE • DRV/r vs LPV/r ARTEMIS
KLEAN KLEAN Study: FPV/r BID vs LPV/r BID,in combination with ABC/3TC • Design Randomisation* 1:1 Open-label W48 N = 434 > 18 years ARV-naïve HIV RNA > 1,000 c/mL Any CD4 cell count N = 444 *Randomisation was stratified on HIV RNA < or > 100,000 c/mL • Objective • Non inferiority of FPV/r vs LPV/r at W48: % HIV RNA < 400 c/mL, ITT, TLOVR algorithm (lower margin of the 95% CI for the difference = - 12%, 90% power) Eron J. Lancet 2006;368:467-82
KLEAN KLEAN Study: FPV/r BID vs LPV/r BID,in combination with ABC/3TC Baseline characteristics and patient disposition Substitution of any NRTI for ABC in case of suspected hypersensitivity; no other ARV substitutions allowed Eron J. Lancet 2006;368:467-82
KLEAN KLEAN Study: FPV/r BID vs LPV/r BID,in combination with ABC/3TC HIV RNA < cut-off at week 48 FPV/r LPV/r % • % HIV RNA < 50 c/mL(ITT-E, TLOVR) wassimilar between FPV/r and LPV/r across baselinesubgroups (low or highHIV RNA, low or high CD4) • Median CD4 increaseat W48: 176/mm3 (FPV/r)vs 191/mm3(LPV/r) • Virologic failures at W48 (TLOVR analysis): 26 (FPV/r) vs 30 (LPV/r), including unconfirmed HIV RNA > 400 c/mL on final visit < 400 c/mL < 50 c/mL < 50 c/mL < 50 c/mL 100 Primary efficacy endpoint 89 88 80 73 71 67 67 66 65 60 40 20 N = 434 444 434 444 328 341 0 ITT-E, TLOVR ITT-E, TLOVR ITT, M/D = F Observed analysis, ITT-E 95% CI for the difference = - 4.8; 7.05 ITT-E : ITT-exposed ITT, M/D = F : ITT missing/discontinuation = failure Eron J. Lancet 2006;368:467-82
KLEAN KLEAN Study: FPV/r BID vs LPV/r BID,in combination with ABC/3TC • Resistance data • Genotypic and phenotypic resistance testing was done at virologic failure: • Viral rebound (2 consecutives HIV RNA > 400 c/mL after achieving < 400 c/mL • HIV RNA > 400 c/mL at W24 * No reduced phenotypic susceptibility, no acquisition of major PI mutations Eron J. Lancet 2006;368:467-82
Safety and tolerability: FPV/r vs LPV/r Similar frequency of premature discontinuations for adverse events: 12% vs 10% Similar frequency of clinical adverse events grade 2 to 4 and laboratory abnormalities grade 3 to 4 in both groups Diarrhoea was the most common adverse event, and led to treatment discontinuation in 1% and 2%, respectively Similar frequency of suspected abacavir HSR: 7% vs 5% Similar frequency of grade 3-4 alanine transaminase (ALT): 12% of patients with hepatitis B and/or C co-infection vs 1% in the absence of co-infection Similar changes in fasting lipids at W48, including triglycerides. Use of lipid-lowering agents during the study period: 11% in both groups KLEAN KLEAN Study: FPV/r BID vs LPV/r BID,in combination with ABC/3TC Eron J. Lancet 2006;368:467-82
KLEAN Study: FPV/r BID vs LPV/r BID,in combination with ABC/3TC KLEAN • Summary - Conclusion • In combination with ABC/3TC QD, FPV/r BID was non inferior to LPV/r BID • Virologic and immunologic outcomes at W48 were similar with FPV/r and LPV/r • In patients with high baseline HIV RNA and those with low baseline CD4, similar antiviral potency of the 2 PI/r was evidenced • Tolerability and safety, numbers of treatment discontinuations, and increases in fasting lipids were similar for FPV/r and LPV/r • Confirmed virologic failure was uncommon in both groups with no emergence of major protease inhibitor-associated resistance mutation in either group • In antiretroviral-naïve patients, FPV/r BID provides similar antiviral efficacy, immunologic response, safety and tolerability as LPV/r, both in combination with fixed dose ABC/3TC QD Eron J. Lancet 2006;368:467-82