Download
1 / 75
780 likes | 1.01k Views
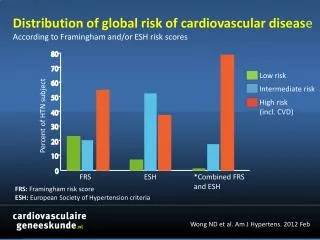
Update on HTN and ABPM. Raj Padwal Division of General Internal Medicine University of Alberta. Disclosures. Funding : CIHR, AIHS, HSF, UHF Research Collaboration : Novo Nordisk, CVRx Consulting : Vivus , Medtronic Speaking and other Honoraria : Abbott. Outline.

E N D
Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta
Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic Speaking and other Honoraria: Abbott
Outline • Understand how to interpret ABPM. • Review the pros and cons of different methods to diagnose hypertension. • Discuss some current controversies in HTN management.
European Society of Hypertension Classification of Blood Pressure The category pertains to the highest risk blood pressure *ISH=Isolated Systolic Hypertension. J Hypertens 2007;25:1105-87.
Hypertension in Canada: Prevalence and Control Overall prevalence is 21% McAlister et al. CMAJ 2011
14 16 18 20 14 16 18 20 0 4 6 8 10 12 0 4 6 8 10 12 2 2 Life time risk of Hypertension in Normotensive Women and Men aged 65 years Risk of Hypertension % Risk of Hypertension % 100 100 Women Men 80 80 60 60 40 40 20 20 0 0 Years to Follow-up Years to Follow-up JAMA 2002: Framingham data.
Standardized Preparation: Patient No acute anxiety, stress or pain. No caffeine, smoking or nicotine in the preceding 30 minutes. No use of substances containing adrenergic stimulants such as phenylephrine or pseudoephedrine (may be present in nasal decongestants or ophthalmic drops). Bladder and bowel comfortable. No tight clothing on arm or forearm. Quiet room with comfortable temperature Rest for at least 5 minutes before measurement Patient should stay silent prior and during the procedure. Blood Pressure Assessment:Patient preparation and posture
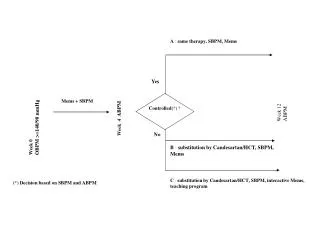
Clinic BP ABPM (If available) Home BPM Hypertension visit 3 >160 SBP or >100 DBP Diagnosis of HTN >135/85 Awake BP <135/85 and 24-hour <130/80 Awake BP >135 SBP or >85 DBP or 24-hour >130 SBP or >80 DBP < 135/85 <160 / 100 ABPM or HBPM or Hypertension visit 4-5 >140 SBP or >90 DBP Diagnosis of HTN Diagnosis of HTN Continue to follow-up Continue to follow-up Diagnosis of HTN Continue to follow-up < 140 / 90 II. Criteria for the diagnosis of hypertension and recommendations for follow-up BP: 140-179 / 90-109 Confirm with repeat Home BPM or ABPM Patients with high normal blood pressure (clinic SBP 130-139 and/or DBP 85-89) should be followed annually.
Clinic, Home, Ambulatory (ABP) Blood Pressure Measurement Equivalence Numbers A clinic blood pressure of 140/90 mmHg has a similar risk of a:
ABPM Indications Chughtai and Peixoto. Hosp Phys 2003
Contraindications to ABPM • Not cooperative • Severe PVD or thrombocytopenia • Afib (relative): not accurate • Arm too big • Severe office HTN (≈220/120)
Information Provided by ABPM • Estimate of true overall 24 hour BP • Diurnal variation in BP • Variability in BP • Duration of action of drug
ABPM Normal Parameters BP should dip by 10-20% during sleep Chughtai and Peixoto. Hosp Phys 2003
ABPM: Number of Readings • Recommendation is at least 14 readings in the daytime (NICE Guidance). • Minimum number is 2 per hour. • We usually do a reading an hour at night.
ABPM 5 Ziemmsen. J NeurolSci 2010
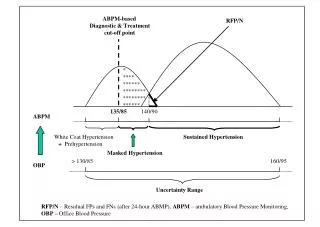
135 White Coat and Masked Hypertension 200 180 Masked Hypertension Hypertension 160 Home/Ambulatory SBP mmHg 140 120 White Coat Hypertension Normotension 100 100 120 140 160 180 200 Office SBP mmHg Derived from Pickering et al. Hypertension 2002: 40: 795-796
Prognosis of Masked Hypertension Prevalence of masked hypertension is approximately 10% in the general population but is higher in patients with diabetes J Hypertension 2007;25:2193-98
Prognostic Significance of Clinic vs. ABPM Dawes. BP Monit 2006
Prognostic Significance of Clinic vs. ABPM Dawes. BP Monit 2006
Diagnostic Utility of BP Measures NICE 2011 Guidance Document
Diagnostic Utility of BP Measures Hodgkinson. BMJ 2011
Cost-Effectiveness of ABPM Lovibond. Lancet 2011
Diagnosis of Hypertension: Key Points • Non-automated office BP measurements are not accurate. • This results in inappropriate management. • Out-of-office measurement – particularly ABPM – should be used to confirm the diagnosis of HTN.
Predictive Role of Nighttime BP Hansen. Hypertension 2012
MAPEC Hypothesis: Bedtime chronotherapy leads to better BP control and reduces CV endpoints. Design: PROBE RCT Country: Spain Sample Size: 2156; mean age 56 Endpoints: • All-cause mortality and CVD events (huge composite endpoint) • 48-hour ABPM
MAPEC: Results Baseline awake systolic ABPM was 134 mm Hg. Baseline asleep systolic ABPM was 123 mm Hg.
MAPEC Study: Issues • Inconsistent numbers presented across trial publications. Is this truly an RCT with a predefined start and end? Original sample size in the protocol was 3344. Subsequent publication mentions 734 normotensive subjects – uncertain if they are included in the main paper. • Most of the literature in the field comes from a single centre and one group of investigators. • Huge effect size from such a small, simple change.
Bottom Line: Bedtime Dosing • Practical point: relatively simple ‘intervention’ • Conversely, I don’t view the data as definitive yet. • I don’t routinely do it; however, I will in refractory hypertension. Also, in this group, I often use drugs that need bedtime dosing (alpha blockers and some CCBs).
Choice of ‘Thiazide’ Diuretic for HTN Chlorthalidone vs. HCTZ
Pharmacologic Structure • Chlorthalidone is often mislabeled as ‘thiazide-like’. • It is a non-thiazide with a distinct pharmacological structure…. • ….that has similar pharmacological action (DCT NaClsymporter blockade) Kurtz. Hypertension 2012.
Thiazides and Non-thiazides Thiazides Hydrochlorothiazide Chlorothiazide Methychlothiazide Polythiazide Bendroflumethiazide Non-thiazides Chlorthalidone Indapamide Metolazone
Pharmacokinetics Carter BL. Hypertension 2004;43:4-9
BP Control • Meta-analysis of 108 HCTZ and 20 chlorthalidone studies (n=10443) • Comparisons are indirect, not head-to-head • Chlorthalidone is a more potent drug Dose Ernst, ME. Am J Hypertens. 2010
MRFIT Trial Results MRFIT. JAMA 1986
Diuretic Choice: Summary • Thiazides and non-thiazides are similar and dissimilar properties. • Chlorthalidone (non-thiazide) is more potent and can reduce BP more than HCTZ at equal doses. • Non-definitive ‘hard outcome’ indirect comparisons: ?chlorthalidone better