Download
1 / 21
400 likes | 1.07k Views
EMS CPAP. Concepts and Use Presented and adapted by Todd Lang, MD. Goals. Improve survival Stabilize patient/relieve symptoms Decrease need for other interventions By EMS In ED Specifically, intubations Decrease ICU (and transfers out of area). EMS CPAP.

E N D
EMS CPAP Concepts and Use Presented and adapted by Todd Lang, MD
Goals • Improve survival • Stabilize patient/relieve symptoms • Decrease need for other interventions • By EMS • In ED • Specifically, intubations • Decrease ICU (and transfers out of area)
EMS CPAP • Reasonably well studied and seems to: • Be safe—very rare complications, EMT-B in MI, WI • Be effective—several studies show effects above both pre- and in-hospital • Boussignac device seems to be best current option to decrease up front cost for this rare intervention
CPAP vs. Intubation CPAP • Non-invasive • Easily discontinued • Easily adjusted • Use by EMT-B • Minimal complications • Does not require sedation • Comfortable Intubation • Invasive • Intubated stays intubated • Requires highly trained personnel • Significant complications • Can require sedation or RSI • Potential for infection
CPAP avoids RSI • Conscious patients • Transient intervention • In the “pre-crash” phase of illness • No risk of complications that RSI brings • No downstream healthcare implications like intubation/RSI • Easier to do with limited people
Physiology of CPAP • Airway pressure maintained at set level throughout inspiration and expiration • Maintains patency of small airways and alveoli • Improves gas exchange • Improves delivery of bronchodilators • Moves extracellular fluid into vasculature • Reduces work of breathing
Adult Respiratory Distress (Age greater than 12) Routine Medical Assessment Oxygen 2 LPM via Nasal Cannula Titrate to maintain Pulse ox of >92% • Is Patient a candidate for Mask CPAP? • Respiratory Rate > 25 / min • Retractions or accessory muscle use • Pulse ox < 94% at any time Yes See CPAP Protocol No Is the Patient wheezing and/or does the Patient have a history of Asthma/COPD? Yes Administer Albuterol / Atrovent by Nebulizer No Does the Patient have rales and/or does the Patient have a history of congestive heart failure (CHF)? Contact Medical Control, consider sublingual NTG if systolic BP is >100mmHg, possible furosemide if long transport Yes No Contact Medical Control
Mask CPAP for EMS Asses Patient, record vital signs and pulse ox before applying oxygen • CPAP Inclusion Criteria • (2 or more of the following) • Retractions or Accessory muscle use • Respiratory Rate > 25 / minutes • Pulse Ox < 94% at any time • CPAP Exclusion Criteria • -Unable to follow commands • Apnea • Vomiting or active GI bleed • Major trauma / pneumothorax • Conditions Indicated for CPAP • Congestive Heart Failure • COPD / Asthma • Pneumonia Does the Patient meet two or more Inclusion Criteria? No Yes Yes Does the Patient meet any Exclusion Criteria? Continue standard Respiratory Distress Protocol No Administer CPAP 5 cm H2O of pressure AND Reassess patient, vital signs, and respiratory distress scale every 5 min. Patient condition is deteriorating Decreasing LOC Decreasing Pulse Ox Patch to Medical Control Respiratory Distress Protocol Patient condition is stable or improving Continue CPAP Reassess patient every 5 minutes Notify Medical Control Complete Airway Data Form and submit PHC for each patient placed on CPAP Remove CPAP Apply BVM Ventilation
Indications for CPAP • CHF • Pulmonary Edema • Near Drowning • Inhalation Exposure • COPD • Asthma • Pneumonia
Contraindications • Code/cardiac arrest • Trauma to face • Unable to get a seal with mask • Pneumothorax • Vomiting/upper GI bleeding • Patient intolerance (despite treatment with midazolam)
Items to Consider • Oxygen supply is rapidly depleted at higher pressure rates • Pressure level • Most studies show 5cm H20 sufficient • Complication rate goes up with pressure • 5cm is probably best place to start EMS CPAP and titrate if needed from there
Summary • CPAP is a non-invasive procedure that is easily applied and can be easily discontinued without untoward patient discomfort • Data supports its use in CHF, pulmonary edema, COPD/Asthma, and pneumonia • Data support EMS CPAP use and its safety and benefits to patients
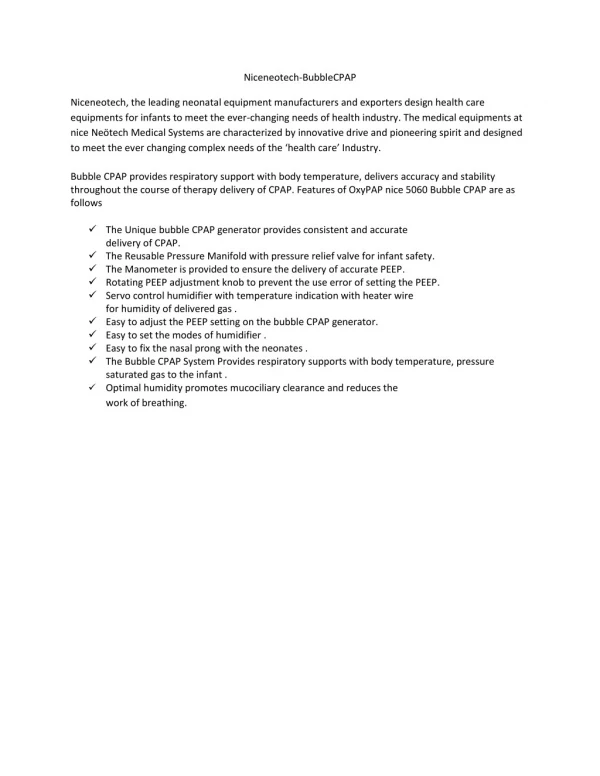
Boussignac CPAP System • Select the appropriate size face mask for your patient: - Child Mask (Size 3) - Small Adult Mask (Size 4) - Medium Adult Mask (Size 5) - Large Adult Mask (Size 6)
Boussignac CPAP System • Set Oxygen flow to deliver CPAP in cmH2O of water pressure: - 15 liters = 5cmH2O - 20 liters = 7.5 cmH2O - 25 liters = 10 cmH2O
Boussignac CPAP System • Attach the head strap to the hook rings on one side of the Boussignac CPAP mask. • Explain to the patient how the Boussignac CPAP will help their breathing. • Gently hold the mask to the patients face insuring a good face/mask seal. • Turn the flow control device to the desired liters/min, generally 15 l/min, to begin the CPAP. • Gradually adjust the flow to achieve the desired level of CPAP.
Boussignac CPAP System • Move the head strap around the patient’s head. Insure that the round disk on the head strap is located on the crown of the patient’s head. Attach the head strap on the hook rings. • Check around the mask for any leaks. • Adjust the mask and/or head strap accordingly to insure the patient’s comfort. • Monitor patient’s vital signs.
Boussignac CPAP System • If the patient requires suctioning of the oral cavity, insert French size suction catheter through the open end of the Boussignac CPAP System. • CPAP pressure will not be affected.
Boussignac CPAP System + Nebulizer • Fill the nebulizer with the prescribed medication.
Boussignac CPAP System + Nebulizer • Insert the 22 mm male end of the nebulizer into the face mask. • Insert the 22 male end (white) of Boussignac CPAP into the nebulizer. • Monitor patient’s vital signs.
Boussignac CPAP System + Nebulizer • Connect the funnel end of the nebulizer’s gas delivery tube to a gas source. • Turn on gas source to 6 liters/min. to power the nebulizer. • Maintain O2 flow to Boussignac CPAP System at 15 l/min. (5cmH2O).