Download
1 / 28
280 likes | 704 Views
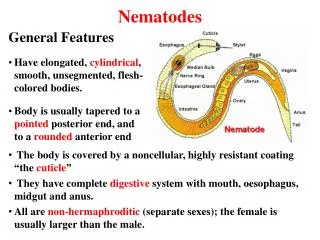
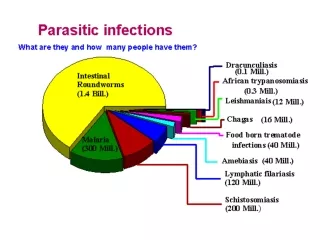
Chapter 29 - Nematodes: Filaroidea. Generalized Life Cycle The long thread-like, adult filarial worms are found in the lymphatic glands, tissues and body cavities of the host Females are ovoviparous, with larvae hatching in the uterus.

E N D
Generalized Life Cycle • The long thread-like, adult filarial worms are found in the lymphatic glands, tissues and body cavities of the host • Females are ovoviparous, with larvae hatching in the uterus • At the time of larviposition, the larvae, known as microfilariae, are less well developed than typical first stage larvae and are considered prelarvae or advanced embryos • Once deposited, microfilariae migrate into the blood vessels (via the thoracic lymph duct or by penetrating the walls of the lymph vessels) to invade neighboring small blood vessels
Generalized Life Cycle cont. • Larvae can survive in the blood for years until ingested by the insect vector • Blood inhabiting microfilariae are usually sheathed, retaining the flexible eggshell as an outer covering • However, in tissue dwelling species, the sheath is usually sloughed and the larvae is said to be unsheathed
Generalized Life Cycle cont. • After being ingested in a blood meal of a suitable insect vector, microfilariae develop in the digestive tract of the insect into the first stage, rhabditiform larvae • These larvae penetrate the midgut into the homocoel and migrate into the thoracic muscles where the molt and metamorphose into the infective 3rd stage filariform larvae • Filariform larvae migrate to the proboscis of the insect and get into the human blood stream while the insect is feeding
Generalized Life Cycle cont. • In the human, larvae undergo molts and metamorphose into adult worms during their migration to the definitive site of infection • Within about 6 months microfilariae appear in the blood stream
Periodicity • There is usually a nocturnal surge in the microfilarial population in the peripheral circulation • The nature of the periodicity varies among species and even among strains • For example, while microfilariae of W. bancrofti in the Caribbean, SA, Africa, and Asia are nocturnal, those of the strain endemic to the South Pacific Islands are diurnally subperiodic (they are present in the peripheral circulation throughout a 24 h period, their numbers increase during the day time) • When the microfilarial worms vacate the peripheral circulatory system, they accumulate in the small vessels of the lungs and liver
Periodicity cont. • Evolution of the phenomenon is of obvious survival value since it enhances opportunity for microfilariae to be ingested by the insect vectors at certain times • It is not surprising that the surge of microfilariae coincides with the active feeding periods of the various insect vectors • The mechanism responsible for microfilarial periodicity is uncertain • However, it is known that it is dependent on the 24 h activity pattern (=circadian rhythm) of the definitive host • The sleeping period of the host is characterized by decreases in body temperature and oxygen tension, increases in carbon dioxide tension and body acidity, etc. • Any of these physiological changes may trigger the rhythmic behavior of the microfilariae
Wuchereria bancrofti • This filarial worm is parasitic only to humans • It is characterized by extensive enlargement of extremities • Ancients likened the thickened skin to that of elephants, hence the misnomer elephantiasis (which literally means “caused by elephants” rather than “like elephants”)
Life Cycle • Adults lived coiled together in the major lymphatic ducts • Here the lymph vessels and glands become blocked causing edema • In time, the accumulation of connective tissue cells and fibers contributes to the enlargement of limbs, scrotum, and other extremities
Life Cycle cont. • Sheathed microfilariae, following deposition, utilize mosquitoes (Culex, Aedes, Anopheles) as vectors • Once introduced into the definitive host, larvae migrate to various lymphatics of the groin glands and epididymis of males and labial and mammary glands of females
Epidemiology • Widely distributed: Nile delta, central Africa, Turkey, India, southeast Asia, Pacific Islands, and parts of SA e • Human infections are closely related to the ecology of the mosquito vectors as well as to human habits
Clinical Features • Lymphatic filariasis most often consists of asymptomatic microfilaremia. • Some patients develop lymphatic dysfunction causing lymphedema and elephantiasis, frequently in the lower extremities (including scrotal elephantiasis). • Laboratory Diagnosis • Identification of microfilariae by microscopic examination of blood is the most practical diagnostic procedure. • Treatment • Use of antibacterial cream on wounds stops bacterial infections and keeps swelling from worsening. • Diethylcarbamazine (under an investigational New Drug Protocol from the CDC Drug Service) and ivermectin are effective for the treatment of filariasis.
Brugia malayi • Until 1960 several species of filarial worms with similar microfilariae were assigned to the genus Wuchereria • However, in that year, based on the study of adult worms, the genus Brugia was established to designate the “malayi” group, including Brugia malayi • Its life cycle closely parallels that of W. bancrofti • While B. malayi rarely affects the genitalia, the adult worms live in the lymphatic system and otherwise cause the same symptoms as W. bancrofti, culmanating in elephantiasis
Onchocerca volvulus • Most prevalent in tropical Africa, central and SA and Mexico • Adult worms are found in fibrous nodules located under the skin called onchocercomas in the subcutaneous connective tissues and viscera of humans • Location of the nodules differs according to geographic areas, which in turn may be correlated with the biting preferences of insect vectors • Usually there is a male and a female coiled in each nodule, but occasionally several worms are observed coiled within a single onchocercoma Cross-section of fibrous nodules showing worms
Symptomology • The microfilariae can invade the cornea and cause inflammation of the sclera, cornea, iris and retina • Formation of fibrous tissue usually follows, leading to impaired vision or total blindness = river blindness • The presence of microfilariae in the connective tissues of the skin often produces severe dermatitis resulting from either allergic responses (inflammatory response) or toxicity • Affected areas of the skin become thickened, depigmented, wrinkled and cracked • Symptoms which resemble vitamin A deficiency, suggesting that the parasites’s compete with the host for vitamin A • Adult worms may also cause subcutaneous nodules, especially over bony prominences
Symptomology cont. Patient with river blindness Patient suffering from severe dermatitis
Loa loa • Because their movement is often visible beneath the conjunctival epithelium, these parasites are known as African eye worms • Humans and baboons are the only definitive hosts for Loa loa • The microfilariae are diurnal in the peripheral blood, retreating to the capillaries of the lungs at night • The disease is mainly limited to African equatorial rainforests and southern Sudan • The intermediate hosts (mango fly genus Chrysops) breed in muddy ponds and swamps; thus there is a high incidence of infection in those kinds of habitats
Symptomology • It is only mildly pathogenic • Adult worms migrate through the subcutaneous tissues of the body, moving through the tissues at a maximum rate of about 1.5 cm/min • The most troublesome infection sites are the conjunctiva where impaired vision, irritation and pain may result • Most symptoms are general inflammatory reactions to adults and microfilariae • A typical manifestation takes the form of transient, painful, subcutaneous swellings, commonly referred to as fugitive or Calabar swellings (develop when the worm is still, disappear when they move on) • These are most often seen on the hands or forearms or near the eyes
Symptomology cont. Adult Loa loa coilied under the conjunctival epithelium of the eye Adult Loa loa visible under the skin
O. Spirurida • S.O. Camallanina • This suborder differs in important ways from the suborder Spirurina • It has conspicuous phasmids with broad cavities and prominent pores • The esophageal glands are uninucleate • The intermediate hosts are copepods
Dracunculus medinensis - The Guinea Worm • Dracunculiasis (guinea worm disease) • An ongoing eradication campaign has dramatically reduced the incidence of dracunculiasis, which is now restricted to rural, isolated areas in a narrow belt of African countries and Yemen.
Life Cycle • Humans become infected by drinking unfiltered water containing copepods (small crustaceans) which are infected with larvae of D. medinensis . • Following ingestion, the copepods die and release the larvae, which penetrate the host stomach and intestinal wall and enter the abdominal cavity and retroperitoneal space .
After maturation into adults and copulation, the male worms die and the females (length: 70 to 120 cm) migrate in the subcutaneous tissues towards the skin surface . • Approximately one year after infection, the female worm induces a blister on the skin, generally on the distal lower extremity, which ruptures.
When this lesion comes into contact with water, a contact that the patient seeks to relieve the local discomfort, the female worm emerges and releases larvae . • The larvae are ingested by a copepod and after two weeks (and two molts) have developed into infective larvae . • Ingestion of the copepods closes the cycle .
Symptomology • Dracunculus medinensis infections cause a broad spectrum of nonspecific symptoms such as eosinophilia, nausea, diarrhea, asthma, and fainting • They are believed to result from absorption of metabolic wastes produced by female worms during papule formation • In addition, cutaneous ulcers caused by female worms are common sites for bacterial infections • Female worms failing to reach the host skin sometimes cause reactions in deeper tissues of the body • Commonly they degenerate or become calcified • During these processes the worms may release strongly antigenic molecules that can cause fluid abscesses or worms that calcify near a joint may produce arthritis
Treatment • Gravid female worms are commonly drawn out mechanically from the ulcerated area, but this approach requires painstaking care and the worms must be extracted slowly • If the worm breaks during extraction larvae escape into the subcutaneous tissues causing severe and painful inflammation • The ancient method, dating back to biblical days, of rolling the worm on a stick is still used is parts of Africa and Asia • During the procedure the worm is coiled around a stick which is turned slowly withdrawing the worm a few centimeters per day