Download
1 / 27
270 likes | 371 Views
Progress towards interoperability standards for anesthesiology. HL7 UK 2007 Conference – Making Interoperability Work November 22 nd , 2007. Martin Hurrell, Terri Monk, Andrew Norton, Melvin Reynolds APSF - DDTF / IOTA, HL7 SIGGAS, AMS Consulting.

E N D
Progress towards interoperability standards for anesthesiology HL7 UK 2007 Conference – Making Interoperability Work November 22nd, 2007 Martin Hurrell, Terri Monk, Andrew Norton, Melvin Reynolds APSF - DDTF / IOTA, HL7 SIGGAS, AMS Consulting
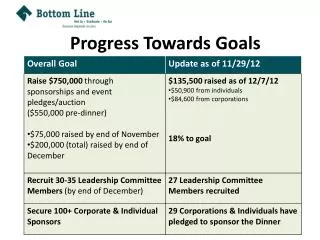
Anesthesiology: what are the drivers ? • The anesthetic record • Medico-legal • ‘On-line’ document • Audit & research • Data sharing • Common record structure : to identify clinical context • Common terminology : for aggregation and analysis • Common model : to enable AI applications, reasoning and decision support
APSF Commitment to AIMS Systems “ The APSF endorses and advocates the use of automated record keeping in the perioperative period and the subsequent retrieval and analysis of that data to improve patient safety ” APSF Board of Directors October 2001
Anaesthesia Information Management Systems(AIMS) • Only installed in 3-5% of US hospitals • Similar picture in the UK • We expect universal implementations in the UK as part of the National Clinical Records Service (NCRS) … but the time scale is unclear • Creating a data dictionary involves a long implementation path and significant cost • Every implementation seems to have its own data dictionary • The “not invented here” syndrome
Intra-operative record • Device monitoring • Fresh gas flow, concentration of inspired agent(s) • Physiological data • BP, HR, SpO2, Temp, ventilation (and many others) • Drugs and fluids • Bolus and infusion drugs, blood products • Anesthetic agents, resuscitation drugs
Demographics (highly structured) Drugs and vital signs (highly structured) Case Events (??unstructured)
Terminology Schema: record structure Ontology: domain model Foundations for future AIMS
Terminology … some issues …
Hospital A Hospital C Hospital B Multicenter study of factors related to tourniquet injuries
DDTF Reference set Anesthesia Subset SNOMED CT The terms are mapped/linked to an existing wider body of work … which is adopted by the medical community DDTF Reference set Used by APSF Corporate partners Relevance of a Data Dictionary
General anaesthesia Local anaesthesia Vascular access procedures Attributes and modifiers for procedures Anaesthetic drugs Fluids and blood products Monitoring terms Anaesthesia equipment Airway management Some administrative terminology Scales and assessments relevant to anaesthesia Positioning and patient protection The October 2007 termset … around 3,500 terms
x73 Nomenclature & IOTA ontology / terminology • “the Systematic Name is an <n>-tuple of a Base Concept and a series of Differentiating Criteria” • IOTA develops and maintains its ontology in OWL DL • IOTA aims to use the x73 base concepts and associated 1st., 2nd. And 3rd. level differentiators in its device and measurement ontology • Concept names will use the x73 ‘Common Term’ and the associated description will be the x73 ‘Description / Definition’ – optionally, synonyms may be defined • x73 Differentiators will be properties of IOTA concepts
The next stages • Completion of pre operative assessment terminology • Terms to support NSQIP (National Surgical Quality Improvement Program) • Specialized terms necessary for anaesthesia subspecialties e.g. • Cardiothoracic, Obstetrics, Neurosurgery, etc. • CDA compliant schema for the anesthetic record • Alignment of device terms with ISO 11073
Current schema-related work • Development of use cases • Modelling of national business practices • Evaluation of current artefacts • Liaison with NSQIP on requirements
Gardner M., Peachey T. A Standard XML Schema for computerised anaesthetic records. Anaesthesia, 2002, 57, pp1174-1182
Image DICOM, JPEG Image Picture CDA Anesthesia record Waveform e.g. ECG MFER LAB Monitoring measurement X.73 With thanks to Masaaki Hirai, Nihon Kohden
Objectives • Why are we even bothering to do outcomes research? • What are the opportunities? • Why now do we want to look at anesthetic data? • Why is it so hard and why have so few people done meaningful research in this area?
National Surgical Quality Improvement Database • 2003 IOM report “Patient Safety, Achieving A New Standard of Care” • national health care infrastructure is needed to “capture patient safety information as a by-product of care and use this information to design even safer delivery systems.” • ACS NSQIP is already capturing information on preoperative patient risk factors, surgical factors, and adverse events following surgery
National Surgical Quality Improvement Database In November 2003, the Institute of Medicine (IOM) released a report entitled, Patient Safety, Achieving A New Standard of Care. In this report, the IOM stated that a national health care infrastructure is needed to “capture patient safety information as a by-product of care and use this information to design even safer delivery systems.” The American College of Surgery National Surgery Quality Improvement Program (ACS NSQIP) program is already meeting one of the IOM recommendations by capturing information on preoperative patient risk factors, surgical factors, and adverse events following surgery. However, the effects of anesthetic management on postoperative outcomes remains unclear largely because the nearly universal method for the documentation of anesthesia has been the paper anesthesia record completed in pen by the anesthesia provider. In recent years, Anesthesia Information Management Systems (AIMS) are being implemented in operating rooms so that accurate intra-operative hemodynamic and anesthetic management information can now be automatically collected. But, thelack of standards in both terminology and record structure prevents the transfer of intra-operative anesthesia data from AIMS into outcomes databases. The creation of a standard terminology and record structure is an essential requirement to support the movement of intra-operative data from AIMS into outcomes databases.
Which data from the anesthetic record should we collect? • “Half the money I spend on advertising is wasted: the trouble is I don’t know which half” • John Wanamaker • In 5 year’s time it is too late to say ‘we should have collected X & Y, they’re beginning to look important’ • Measure twice, cut once – have a sound plan, be standards-based and model future requirements not just those for the short-term
Outcomes research in anaesthesia • Research based on AIMS • Is almost universally restricted to examination of physiological variables • Current lack of structure and standardisation of records and terminology does not support outcomes research • Techniques • Procedures • Therapeutic regimens and drugs etc. etc.
Which data from the anesthetic record should we collect? Reports that say that something hasn't happened are always interesting to me, because as we know, there are known knowns; there are things we know we know. We also know there are known unknowns; that is to say we know there are some things we do not know. But there are also unknown unknowns - the ones we don't know we don't know