Download
1 / 1
10 likes | 640 Views
Enhanced Recovery After Surgery: Assessing Potential Benefit for Gynae-Oncology Patients S HOWDEN 1 , C EKECHI 1 , P SARHANIS 1 , M GROVER 2 , 1 Department of Obstetrics & Gynaecology , 2 Department of Anesthetics; Northwick Park Hospital, Harrow. . Introduction. Results. Discussion.

E N D
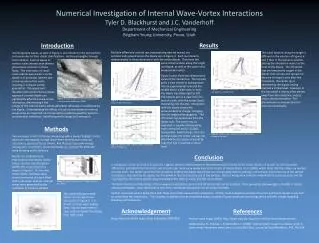
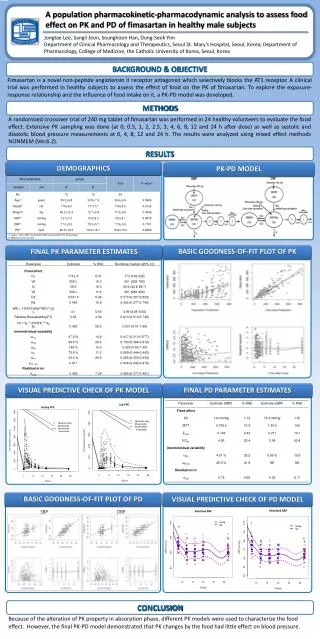
Enhanced Recovery After Surgery: Assessing Potential Benefit for Gynae-Oncology PatientsS HOWDEN1, C EKECHI1, P SARHANIS1, M GROVER2,1Department of Obstetrics & Gynaecology ,2 Department of Anesthetics; Northwick Park Hospital, Harrow. Introduction Results Discussion An example of referral can be improved is a Protocol as in a case study on NHS improvements where a multi disciplinary approach results in patients being transferred from general surgical care to gynaecology at the earliest opportunity. This may reduce time to diagnosis, surgery and morbidity resulting in prolonged admission8 as well as advantages gained due to shorter LOS as above. Enhanced recovery offers the opportunity to improve patient care by optimisation of patient condition prior to surgery, streamlining preoperative investigations and procedures. In turn improving the postoperative period with optimised analgesia, early mobilisation and discharge allow the patient to return to normal life more quickly as well as reducing hospital length of stay. ERAS has been shown to reduce length of stay for surgical patients. In some gynaecological studies this has been up to 28% reduction 1, although less evidence is available for gynae-oncology patients and the largest evidence base is focused on colorectal surgery, 2,3. Although one of the most easily auditable measures length of stay is not the only measure of success in ERAS programmes. Studies show reduced morbidity with ERAS and although data is limited in gynaecology earlier discharges point towards an increased number of readmissions.4 Improving patient involvement in care, education, community support and education (key principles in the ERAS programme) may reduce the effect on this and many general surgical studies including two meta analyses show little effect on readmission rates for ERAS compared to routine post operative pathways.2,3, When considering the whole patient journey overall costs for ERAS patients compared to routine care in colorectal surgery are less. Using 2008-2009 data considering uk figures for hysterectomy (36,500) a potential saving of 34,800 bed days by reducing mean LOS of 4.3 to 3.1.5 Reduced costs free funding for other areas of care for gynae- onc patients. It has been estimated that 30% of women with recurrence of gynae malignancy will present with bowel obstruction,6 these patients as well as those with abdominal pain may be admitted under general surgeons. Prolonged hospital admissions are associated with increased patient morbidity and mortality and increased hospital expenditure. This is most apparent with gynae-oncology patients who may have particularly long hospital admissions. Enhanced recovery after surgery (ERAS) is a perioperative treatment protocol consisting of preoperative (pre operative optimisation and education) intraoperative (anaesthetic and surgical measures) and postoperative (avoidance of opiates, early removal of catheters and mobilisation) designed to reduce patient morbidity and morality as well as inpatient hospital stay reducing costs and improving physical and psychological recovery Conclusion In conclusion for Northwick Park ERAS is not a panacea for reduced length of stay for gynae-oncology patients. To address the patients who have the most protracted inpatient stay a system of rapid referral, investigation, MDT decision making and surgery is necessary to reduce length of stay and its associated sequelae. ERAS may however offer an opportunity to improve peri-operative patient management for elective cases resulting in Improved patient experience and reduced morbidity for these patients. Further measures that could be audited following implementation of ERAS include readmission rate and patient satisfaction. Fig 1. Number of admissions for inpatient surgery by proccedure during Jan/Feb 2010 Objectives The aim of our audit was to assess the post-operative length of stay for the gynae-oncology patients at Northwick Park Hospital prior to a proposed ERAS programme for gynae-oncology patients. The aim of the audit was to identify the current length of stay for these patients to focus enhanced recovery with the intention of reauditing following implementation of an ERAS programme References It was found that the average, post-operative length of stay for the gynae-oncology patients at Northwick Park was 2 days This was due to the majority of procedures performed via the laparoscopic approach. However it was noted that the average length of stay was dependent on the original route of referral, with patients referred via A&E, or via other specialist teams, having a longer than average hospital admission. 18 of the 19 cases were referred via GOPD /rapid access clinic. The single referral from A&E via general surgery had the longest length of stay at 9 days. Fig. 2 Average length of stay for patients admitted for inpatient surgery during Jan / Feb 2010 • Improving quality by introducing enhanced recovery after surgery in a gynaecological department: consequences for ward nursing practice IS Sjetne, U Krogstad, S Ødegård, M E Engh, QualSaf Health Care 2009;18:236-240 • Fast-track vs standard care in colorectal surgery: a meta-analysis update. NikolaosGouvas & Emile Tan & Alistair Windsor & EvaghelosXynos & Paris P. TekkisInt. Journal Colorectal Disease • The enhanced recovery after surgery (ERAS) pathway for patients undergoing major elective open colorectal surgery: A meta-analysis of randomized controlled trials. Krishna K. Varadhan, Keith R. Neal, Cornelius H.C. Dejong, Kenneth C.H. Fearon, OlleLjungqvist, Dileep N. Lobo Clinical Nutrition • 4. Improving patient care with shorter hospital admissions. • Schmid KJ, Tewari R, Nordin AJ. • J ObstetGynaecol. 2009 Aug;29(6):526-8. • 5. The influence of an Enhanced Recovery Programme on clinical outcomes, costs and quality of life after surgery for colorectal cancer. P. M. King, J. M. Blazeby, P. Ewings, R. J. Longman, R. M. Kipling, P. J. Franks, and R. H. Kennedy Colorectal Disease 2006 • 6 Protocol for patients admitted with clinical diagnosis of malignant bowel obstruction secondary to gynaecological cancer • Transforming inpatient care programme case study.http://www.improvement.nhs.uk/cancer/inpatients/wp_case_studies_2010/wp3_royal_cornwall.pdf Methods Patients admitted for surgery under the gynae-oncology team were identified and those undergoing day-case surgery excluded. 19 patients underwent surgery requiring inpatient care. Notes were reviewed to identify procedure, referral route and length of stay. Average length of stay was calculated by procedure and referral route and finding discussed to focus the proposed ERAS pathway to the areas which could most benefit for reduction of length of stay