Download
1 / 1
10 likes | 158 Views
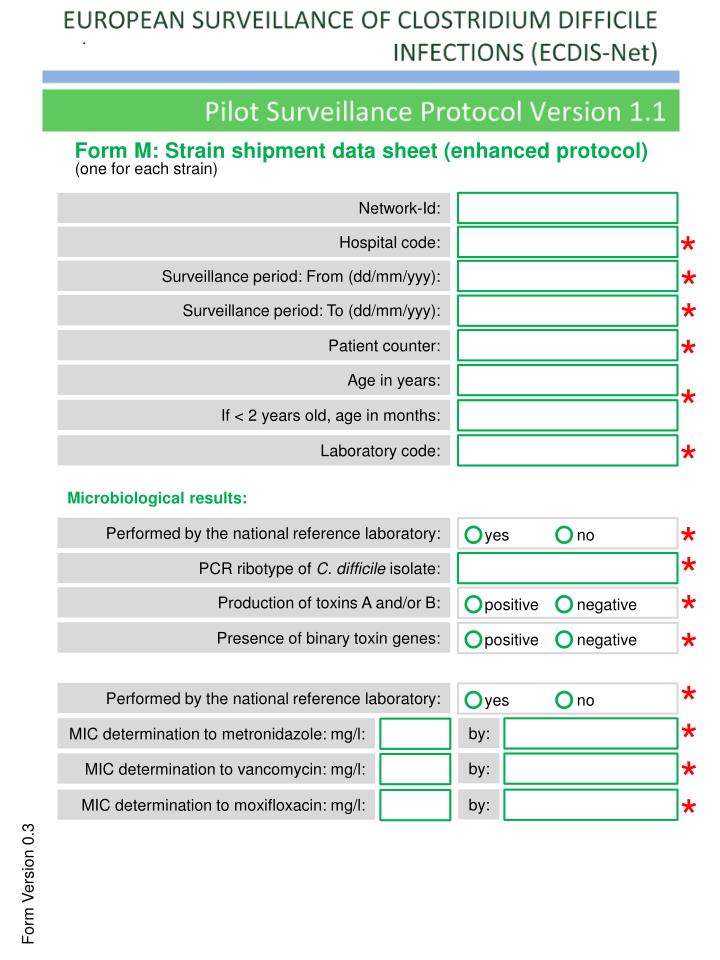
Form M: Strain shipment data sheet (enhanced protocol). ( one for each strain ). Network- Id :. *. Hospital code :. *. Surveillance period : From ( dd /mm/ yyy ):. *. Surveillance period : To ( dd /mm/ yyy ):. *. Patient counter :. yes. yes. positive. positive. no. no.

E N D
Form M: Strain shipment data sheet (enhanced protocol) (oneforeachstrain) Network-Id: * Hospital code: * Surveillanceperiod: From (dd/mm/yyy): * Surveillanceperiod: To (dd/mm/yyy): * Patient counter: yes yes positive positive no no negative negative Age in years: * If < 2 yearsold, age in months: * Laboratory code: Microbiological results: * Performed by the national reference laboratory: * PCR ribotypeofC. difficileisolate: * Productionoftoxins A and/or B: * Presence ofbinarytoxin genes: * Performed by the national reference laboratory: * by: MIC determination to metronidazole: mg/l: * by: MIC determination to vancomycin: mg/l: * by: MIC determination to moxifloxacin: mg/l: Form Version 0.3