Download
1 / 28
• 290 likes • 649 Views
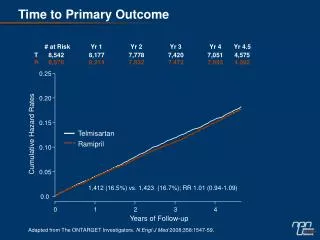
Value of CPET in clinical follow-up. Turkish Thoracic Society Meeting Antalya, Turkey April 2008. Gökhan M. Mutlu, M.D. Pulmonary and Critical Care Medicine Northwestern University Feinberg School of Medicine. Financial Disclosure: Nothing to disclose. CPET: indications.

E N D
Value of CPET in clinical follow-up Turkish Thoracic Society Meeting Antalya, Turkey April 2008 Gökhan M. Mutlu, M.D. Pulmonary and Critical Care Medicine Northwestern University Feinberg School of Medicine Financial Disclosure: Nothing to disclose
CPET: indications • Evaluation of exercise tolerance • Evaluation of undiagnosed exercise intolerance • Evaluation of patients with CV disease • Evaluation of patients with respiratory diseases/symptoms • Preoperative evaluation • Exercise evaluation and prescription for pulmonary rehabilitation • Evaluation of impairment/disability • Evaluation for lung, heart and heart-lung transplantation ATS/ACCP Statement of CPET AJRCCM 2003
CPET: Clinical follow-up indications • LV failure • Clinical follow-up • Evaluation for heart or heart-lung transplant • Monitoring response to treatment • Pulmonary hypertension • Clinical follow-up • Monitoring response to treatment • Chronic pulmonary disease • Before and after exercise training program • Before and after LVRS ATS/ACCP Statement of CPET AJRCCM 2003
CPET: Clinical follow-up indications • Pulmonary rehabilitation • Before and after pulmonary rehabilitation • To determine the exercise prescription and to assess clinical response • Heart and/or lung transplantation • Before and after transplantation ATS/ACCP Statement of CPET AJRCCM 2003
CPET: Clinical follow-up Most commonly used parameters for clinical follow-up • Peak VO2 • AT • VE/VCO2 • O2 pulse • VO2/WR • AT determination is helpful as an indicator of level of fitness, for exercise prescription and to monitor the effect of physical training
Cardiac diseases: LV failure VO2 • the “gold standard” measure of aerobic fitness • Related to the severity of heart failure • Used to stratify risk, guide management and determine exercise training thresholds • >18 ml/kg/min- mild impairment, low risk of CV death in CHF patients • <14 ml/kg/min- indication for heart transplant • <10 ml/kg/min- severe impairment, high risk of CV death. Poor prognosis at 1 year
Cardiac diseases: LV failure VO2 1-year survival >14 ml/kg/min- “too well”- 94% <14 ml/kg/min + accepted for transplant- 48% <14 ml/kg/min + comorbidities- 47% Costanzo MR, et al. Circulation 1995;92:3595-612
Cardiac diseases VE/VCO2
Cardiac diseases: LV failure VE/VCO2 • Normal <29 • VE/VCO2 is inversely related to peak VO2 • Low VE/VCO2 is independently associated with a worse prognosis • Cut-off unclear • ≥35 has been suggested as a predictor
Cardiac diseases: LV failure AT • A surrogate measure of quality of life in patients with CHF • An important marker of outcome
Cardiac diseases: LV failure 6-min walk test (6-MWT) • A submaximal test of functional capacity • Simple to perform • Inexpensive • Tolerable as patients are self-paced during exertion • Reproducible (if well standardized)
Cardiac diseases: LV failure 6-MWT vs CPET (VO2 peak) • Only a moderate relationship • Useful to determine prognosis in CHF • 6-MWT <300 m is a simple and useful prognostic marker of subsequent cardiac death in patients • with severe CHF undergoing evaluation for heart transplantation and • with patients with moderate (NYHA class II-III) systolic heart failure
Diastolic heart failure • The role of CPET is less well studied. • CPET provides similar prognostic information. • Cut-off values are different and depend on the LVEF • Peak VO2 is less valuable compared to VE/VCO2 • VE/VCO2 • 32.6 (EF>40%), 33.1 (>45%) , 33.3 (>50%) Guazzi M, et al. J Am Coll Cardiol 2005;46:1883-90
Pulmonary hypertension CPET vs. 6-MWT There may not be a correlation between CPET and 6-MWT1. Oudiz RJ et al. Am J Cardiol 2006;997:123-6 • 178 patients • ETR antagonist vs. placebo 1. Barst RJ, et al. Am J Respir Crit Care Med 2004;169:441-7 2. Oudiz RJ, et al. Am J Cardiol 2006;997:123-6
Pulmonary hypertension Better correlation when CPET is compared with weight adjusted 6-MWT and at week 12. Oudiz RJ, et al. Am J Cardiol 2006;997:123-6
Pulmonary hypertension American Thoracic Society Guidelines • CPET is recommended for follow-up of PAH patients • 6-MWT is complimentary • CPET is more discriminating • More sensitive at detecting small differences in exercise capacity ATS Statement. AJRCCM 2002;166:111-7
Exercise rehabilitation • Exercise therapy has been recommended for all stable patients with CHF • A systematic review of 81 studies and Meta-analysis of 9 randomized trials. • Exercise training programs are safe decrease mortality from CHF has been shown to improve exercise tolerance Smart N, et al. Am J Med 2004; 116:693-706 Piepoli MF, et al. BMJ 2004;328:189
Exercise rehabilitation VO2 peak • a more accurate marker of exercise tolerance than heart rate • preferable to measure gas exchange during exercise and to prescribe the intensity of the exercise regimen • Healthy: At rate corresponding to 50-70% of VO2 peak • For CHF patients with severe dysfunction- 40-50% of VO2 peak
Exercise rehabilitation The magnitude of improvement in peak VO2 after exercise programs range between 10% and 26% of initial (pre-training) value Statement on CPET in chronic heart failure due to left ventricular dysfunction Eur J of Cardiovasc Prev and Rehab 2006;13:486-94
Peak oxygen consumption in patients with compensated heart failure who did not have exercise training (control group, n = 14) and who did have exercise training (exercise group, n = 15) Keteyian, S. J. et. al. Ann Intern Med 1996;124:1051-1057
Effect of therapy on CPET in CHF Pharmacologic treatment AT1RB ACEI BB VO2 peak ↑ ↑ ↔ VE/VCO2 ↓ ↑ ↓ O2 pulse ↑ ↑ ↑ VO2/WR ↑ ↑ ↔
CPET: Clinical follow-up What is considered significant? • VO2 peak is generally considered reproducible • In order to avoid under and over-estimation with absolute values, changes over time should be expressed as a % of baseline capacity • Variation is influenced by the severity of the condition and interval between tests • Short-term coefficient 4.1%-6%
CPET: Clinical follow-up • To improve reproducibility, the tests should be performed at the same time of the day • Every clinical exercise laboratory should provide short and long-term coefficients of variation of peak and submaximal gas exchange parameters • Another problem area is the correlation between VO2 peak and the subjective clinical exercise tolerance. • Variations of VO2 peak do not necessarily reflect changes in symptom status. • Several studies have shown a non-linear relation between VO2 peak, symptoms and quality of life.