Download
1 / 31
310 likes | 532 Views
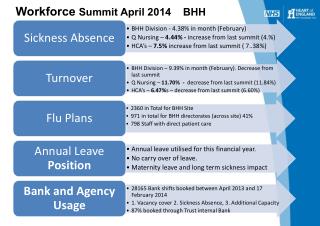
Workforce Summit. Workforce Shortages. Hearings in 1999 MN Psychiatric Study MHAG MH Acute Care Needs Report New Freedom Commission SAMHSA Action Plan for BH Workforce Development. Workforce Shortages. 9 regions of the state designated as MH professional shortage areas

E N D
Workforce Shortages Hearings in 1999 MN Psychiatric Study MHAG MH Acute Care Needs Report New Freedom Commission SAMHSA Action Plan for BH Workforce Development
Workforce Shortages • 9 regions of the state designated as MH professional shortage areas • Only metro area and SE MN not designated • 3 designated in 2012
Workforce Shortages in Every Area • Psychiatrists – 33% fewer per capita than national average, even worse in children’s mental health • Clinical nurse specialists – only 29 practice in children’s mental health
Workforce Shortages in Every Area • Psychologists – 13 counties without any • Clinical Social Workers – 10 counties without any • MH Behavioral Aides – less than 20 in whole state
Workforce Shortages in Every Area • Children • Rural • Culturally specific • Older adult • Co-occuring disorders – SU and health
Individuals Dissatisfied • Lack of quality of workforce • No understanding of recovery • No understanding of resiliencey • No empathy • Blamed parents
Managers Dissatisfied • Unprepared for realities of real-world settings • Unlearn attitudes, practices and assumptions • Little EBP training
Outcomes • Empty beds due to no staff • Over reliance on highest cost care • Prescribing by non MH professionals • Wait lists • Higher case loads • Poor quality
Mental Health Acute Needs Report • 38% had a highly negative impact on services with medical management having the greatest impact. • The lack of qualified applicants and salary/benefits were identified as the top two reasons for vacancies across all programs.
Mental Health Acute Needs Report • Public program reimbursements were seen as a barrier for workforce capacity • Scope of practice issues are linked to funding of training programs. Highly specialized training is required yet those programs are in short supply and not funded adequately. Particularly negative impact in rural areas of the state.
Causes • Low reimbursement rates • Low compensation rates • Required training without salary • Lack of insurance coverage for MH treatment • No connection with agencies • No steps and ladders
Legislation • Hold a summit on workforce issues • Bring together higher ed and mental health • Develop a comprehensive workforce development plan • Submit to legislature Jan 15, 2015
Legislation • Increase the number of MH professionals and practitioners • Ensure appropriate course work & training experience • Increase the number of culturally diverse professionals and practitioners
National Workforce Plan • Insufficient workforce/treatment capacity to meet demand. • The changing profile of the people needing services. • Shift to increased public financing of treatment. • Use of best practices.
Increased utilization of medications in treatment. • Movement toward a recovery management model of care. • Provision of treatment and related services in nonspecialty settings. • Use of performance and patient outcome measures. Discrimination or stigma.
Major Goals Broadening the concept of workforce • GOAL 1: Significantly expand the role of individuals in recovery, and their families when appropriate, to participate in, ultimately direct, or accept responsibility for their own care; provide care and supports to others; and educate the workforce.
Broadening the concept of workforce • GOAL 2: Expand the role and capacity of communities to effectively identify their needs and promote behavioral health and wellness.
Strengthening the workforce • GOAL 3: Implement systematic recruitment and retention strategies at the federal, state, and local levels. • GOAL 4: Increase the relevance, effectiveness, and accessibility of training and education. • GOAL 5: Actively foster leadership development among all segments of the workforce.
Structures to support the workforce • GOAL 6: Enhance the infrastructure available to support and coordinate workforce development efforts. • GOAL 7: Implement a national research and evaluation agenda on behavioral health workforce development.
Workforce Development Plans • 35 states have plans • 7 have good plans – Alaska, California, Connecticut, Missouri, North Dakota, Oklahoma, Virginia
Alaska • Hired a workforce coordinator –shared by DHS, U of Alaska, Alaska MH Trust Authority • Sent faculty to U of South Florida for training in children’s MH
California • Specific goals for diversity • Expand loan repayment and scholarship programs • Promote use of web-based technologies • Partnership between education and mental health
Connecticut • Higher ed curriculum reform • Supervisor skill training • Increase workforce skilled in in-home • Fellowship for faculty in the field
North Dakota • Teach children about mental health career paths • Retention efforts focus on tuition reimbursement and tax incentives
Oklahoma • Special section on cultural competency training
Virginia • Partnerships between community colleges and providers • Incentives for additional training such as flexible work schedules and education leave
Minnesota • Need to review recommendations from MHAG and Mental Health Acute Care Needs Workforce • Regulatory, Reimbursement, Training, Entrance into programs, Preperation, Recruitment, Standardize qualifications, Residency, Internships
Minnesota Efforts in 2013 • MH Behavioral Aides II • Family Peer Specialists • Consultation by psychologists • MERC Funding for psychologists, clinical social workers • Foreign trained professionals expanded to mental health professionals
Next Steps • Plan the summit to ensure excellent participation across areas • Develop a framework to ensure a workforce development plan is written
NAMI Minnesota 800 Transfer Road, Suite 31 St. Paul, MN 55114 651-645-2948 1-888-NAMI-HELPS www.namihelps.org