Download
1 / 1
20 likes | 149 Views
Practical Feasibility of Screening for Critical Congenital Heart Disease in Newborns With Pulse Oximetry A de-Wahl Granelli 1 , M Mellander 1 , J Sunnegårdh 1 , K Sandberg 2 , I Östman-Smith 1 Department of Paediatric Cardiology 1 , Department of Neonatology 2 ,

E N D
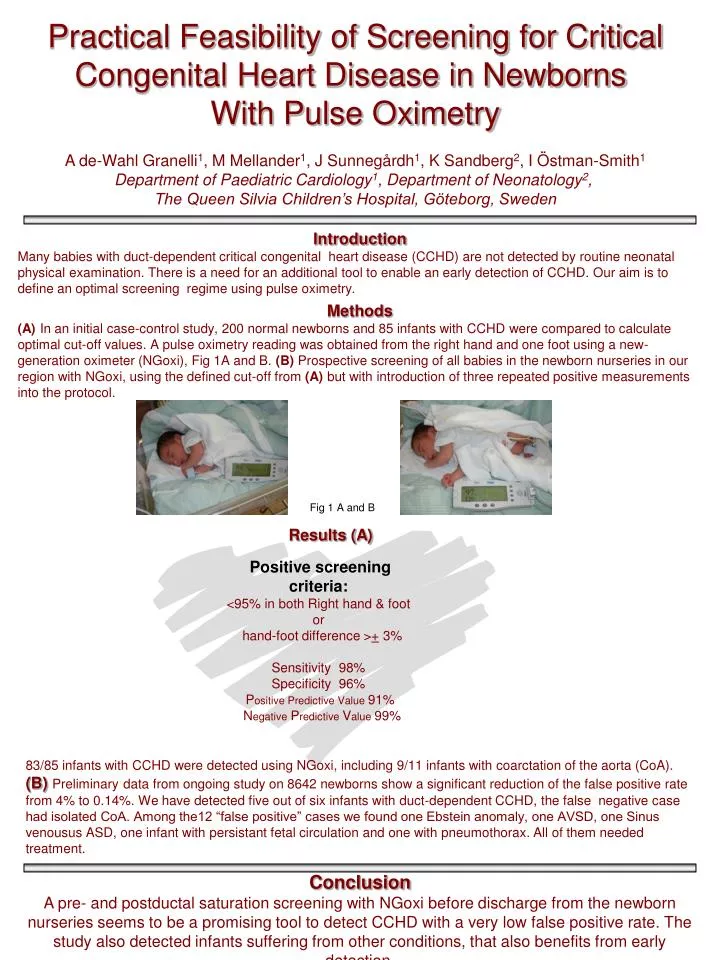
Practical Feasibility of Screening for Critical Congenital Heart Disease in Newborns With Pulse Oximetry A de-Wahl Granelli1, M Mellander1, J Sunnegårdh1, K Sandberg2, I Östman-Smith1 Department of Paediatric Cardiology1, Department of Neonatology2, The Queen Silvia Children’s Hospital, Göteborg, Sweden Introduction Many babies with duct-dependent critical congenital heart disease (CCHD) are not detected by routine neonatal physical examination. There is a need for an additional tool to enable an early detection of CCHD. Our aim is to define an optimal screening regime using pulse oximetry. Methods (A) In an initial case-control study, 200 normal newborns and 85 infants with CCHD were compared to calculate optimal cut-off values. A pulse oximetry reading was obtained from the right hand and one foot using a new-generation oximeter (NGoxi), Fig 1A and B. (B) Prospective screening of all babies in the newborn nurseries in our region with NGoxi, using the defined cut-off from (A) but with introduction of three repeated positive measurements into the protocol. Fig 1 A and B Results (A) Positive screening criteria: <95% in both Right hand & foot or hand-foot difference >+ 3% Sensitivity 98% Specificity 96% Positive Predictive Value 91% Negative Predictive Value 99% 83/85 infants with CCHD were detected using NGoxi, including 9/11 infants with coarctation of the aorta (CoA). (B)Preliminarydata from ongoing study on 8642 newborns show a significant reduction of the false positive rate from 4% to 0.14%. We have detected five out of six infants with duct-dependent CCHD, the false negative case had isolated CoA. Among the12 “false positive” cases we found one Ebstein anomaly, one AVSD, one Sinus venousus ASD, one infant with persistant fetal circulation and one with pneumothorax. All of them needed treatment. Conclusion A pre- and postductal saturation screening with NGoxi before discharge from the newborn nurseries seems to be a promising tool to detect CCHD with a very low false positive rate. The study also detected infants suffering from other conditions, that also benefits from early detection.