Download
1 / 54
540 likes | 701 Views
“Don’t Drink the Water”: A Primer on Infectious Diarrhea. Patty W. Wright, MD with appreciation to Ban Allos, MD March 2011. Objectives. To familiarize participants with the causes, diagnostic work-up, and treatment of the most common etiologies of infectious diarrhea.

E N D
“Don’t Drink the Water”: A Primer on Infectious Diarrhea Patty W. Wright, MD with appreciation to Ban Allos, MD March 2011
Objectives • To familiarize participants with the causes, diagnostic work-up, and treatment of the most common etiologies of infectious diarrhea.
Foodborne-related Illness and Death in the U.S. Events per year Number Illnesses >76 million Hospitalizations >325,000 Deaths >5,000
Salmonella Campylobacter Shigella Listeria Vibrio E. coli O:157 Bacillus Clostridium S. aureus Rotaviruses Norwalk-like viruses Cyclospora Isospora Cryptosporidium Giardia Common Food- and Water-borne Pathogens Causing Diarrhea in the US
Case 1 • A 19 year old female college student presents to the ED at 5 pm c/o the acute onset of N/V with abdominal cramps and mild diarrhea. She denies associated fevers. She ate at a local restaurant today at noon. She reports that several of her classmates have been ill over the past week with the “stomach flu”.
Case 1 • What pathogens are on your differential? • What diagnostic work-up would you perform? • How would you treat the patient?
Acute N/V +/- Diarrhea: Pathogens • Pathogens that have preformed toxins • Cause onset of symptoms within 1-6 hours of ingestion • S. aureus • Bacillus cereus (short-incubation) • “Winter Vomiting Disease” • Norwalk-like viruses • Rotavirus
Acute N/V +/- Diarrhea:Dx and Rx • Typically resolves within 12-24 hrs, without specific therapy • No diagnostic work-up required • Treat with anti-emetics and hydration, if needed
Classic Association/Outbreak • Staphylococcus aureus – ham, cream-filled pastries
Classic Association/Outbreak • Norwalk-like viruses – cruise ships, raw seafood
Case 2 • A 45 year old male develops nausea, diarrhea, and abd cramps at bedtime. He denies any associated vomiting, fever, or blood in his stool. He reports that a friend from work, who at lunch with him at a local Chinese restaurant, is also ill with similar symptoms.
Case 2 • What pathogens are on your differential? • What diagnostic work-up would you perform? • How would you treat the patient?
Acute Diarrhea w/o Vomiting/Fever • Pathogens that produce toxins in vivo • Bacillus cereus (long-incubation) • Clostridium perfringens • Typically resolves within 24 – 48 hrs, without specific therapy • No diagnostic work-up required • Treat symptomatically
Classic Association/Outbreak • Bacillus cereus – fried rice
Case 3 • A 56 year old male with HTN presents to the clinic with a 2 day h/o diarrhea, abd cramps, and fever to 101. He denies blood in his stool or N/V. His wife also reports diarrhea over the past 24 hours. He denies any recent hospitalizations or antibiotic usage.
Case 3 • What pathogens are on your differential? • What diagnostic work-up would you perform? • How would you treat the patient?
Acute Diarrhea and Fever w/o Bloody Stool • Pathogens that cause tissue invasion • Salmonella • Shigella • Campylobacter • Vibrio • Invasive E coli • Listeria
Acute Diarrhea and Fever w/o Bloody Stool • For diarrhea > 1 day in duration or severe (dehydration, fever, blood) • Obtain additional exposure history • Check fecal WBC • If + fecal WBC • Stool culture for pathogens • Consider testing for C diff toxin • Consider empiric abx (adults only)
Acute Diarrhea and Fever w/o Bloody Stool • Treatment: • Hydration • Quinolones typically empiric treatment of choice for food-borne diarrhea • Azithromycin is alternative if cannot take quinolones or risk of resistant Campylobacter
Classic Association/Outbreak • Salmonella – peanut butter
Classic Association/Outbreak • Salmonella and Campylobacter – poultry and poultry products
Classic Association/Outbreak • Vibrio – raw oysters (or wading in the Gulf of Mexico), especially in patients with hepatic dysfxn
Classic Association/Outbreak • Listeria – refrigerated food items (cold cuts, prepared salads), soft cheeses
Classic Association/Outbreak • Shigella – low infectious dose (10-100 organisms), “cool, moist foods that require much handling after cooking”,
Classic Association/Outbreak • Yersinia – pork, chitterlings
Case 4 • A 23 year old female presents to the ED with 3 days of diarrhea. She reports that she initially had watery diarrhea, but that it has now turned grossly bloody. She reports severe abd cramps. She denies fever or N/V.
Case 4 • What pathogens are on your differential? • What diagnostic work-up would you perform? • How would you treat the patient?
Acute Bloody Diarrhea +/- Fever • Pathogens that produce shiga toxin • Shigella dysenteriae • E coli O157:H7 • Evaluation: • Fecal WBC • Stool culture for pathogens (including E coli O157:H7) • Consider testing for C diff toxin • CBC with diff, BMP
Acute Bloody Diarrhea +/- Fever • Treatment • NaCl hydration and supportive care • AVOID antibiotics (especially trim-sulfa) • AVOID antimotility agents in all patients with diarrhea and • High fever or • Bloody diarrhea or • Fecal WBC’s
Hemolytic Uremic Syndrome (HUS) • Occurs in about 10% of pts with E coli O157:H7 • Begins ~ 5-10 days after symptom onset • Triad of microangiopathic hemolytic anemia, thrombocytopenia, and acute renal failure • Most common in kids < 4 yrs old • Mortality rate 5-15% • Older children and adults have poorer prognoses • Na load most protective factor in the prevention of HUS in pts with E coli O157:H7
Classic Association/Outbreak:E. coli O157:H7 1. Food -Foods of bovine origin (hamburger, milk, etc.) -Fruits (apple cider) and vegetables contaminated with manure
Classic Association/Outbreak:E. coli O157:H7 2. Water -Contaminated drinking water -Swimming in contaminated pools and lakes 3. Direct person-to-person or animal-to-person spread -Daycare centers -Long-term care facilities -Petting zoos
Case 5 • A 37 year old male presents to the clinic c/o 4 weeks of daily diarrhea with associated anorexia, fatigue, bloating, and nausea. He denies fevers, vomiting, or blood in his stool. He has lost about 7 pounds over the past month. He denies recent travel.
Case 5 • What pathogens are on your differential? • What diagnostic work-up would you perform? • How would you treat the patient?
Chronic Diarrhea (Non-bloody) • Etiologies • Parasites • Tropical Sprue • Bacterial overgrowth syndromes • Non-infectious causes • Food allergies • Neoplasm and endocrine processes • Functional disorders
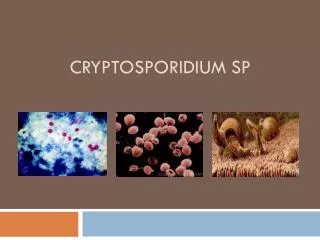
Chronic Diarrhea (Non-bloody) • Most common parasitic causes in US • Giardia • Cryptosporidium • Cyclospora • Isospora Giardia photos: http://phil.cdc.gov/phil/details.asp
Chronic Diarrhea (Non-bloody) • Diagnosis: • Fecal WBC • Wet mount for ova and parasites • Modified acid-fast stain to detect • Cyclospora • Isospora • Cryptosporidium • Giardia antigen testing (stool) • HIV antibody testing • Treatment specific for pathogen isolated
Classic Association/Outbreak • Cryptosporidium – drinking water contaminated with manure after flooding • Cyclospora – raspberries contaminated with bird feces
Chronic Bloody Diarrhea • Inflammatory Bowel Disease (ulcerative colitis or Crohn's disease) most common cause • Differential includes bowel ischemia, colon cancer, or polyps • Infectious causes possible, but much less likely
Case 6 • A 68 year old female with chronic sinusitis presents with fever to 100.7, malaise, abdominal pain, and severe diarrhea which started yesterday. She reports having 20 watery, non-bloody stools since her diarrhea began. Her current medications include a steroid nasal spray, loratidine, and omeprazole.
Case 6: • What pathogens are on your differential? • What diagnostic work-up would you perform? • How would you treat the patient?
Clostridium difficile- Associated Disease • Risk Factors for CDAD: • Antibiotic exposure • Any abx within the prior 2 months • Prolonged hospitalization • Severity of underlying disease • Age > 65 years • GI surgery • PPI
Clostridium difficile- Associated Disease • Spectrum of Disease • Asymptomatic carrier • Diarrhea without colitis • Colitis without pseudomembranes • Pseudomembranous colitis • Fulminant colitis
Clostridium difficile- Associated Disease • Pseudomembranous Colitis www.faculty.plattsburgh.edu
Clostridium difficile- Associated Disease • Fulminant colitis • About 3% of cases • Signs and Symptoms • Diffuse abd tenderness/distention, diarrhea, low BP, high fever, leukocytosis • Complications • Ileus, toxic megacolon, bowel perforation, death
Clostridium difficile- Associated Disease • Diagnosis • ELISA testing for toxins A and B • May need to repeat to improve sensitivity • Cytotoxicity assays • “Gold Standard”, but expensive & requires 48 hrs • Culture for C. diff • Does not distinguish disease from colonization • Colonoscopy • Risk for perforation
Clostridium difficile- Associated Disease • Treatment of mild disease • Metronidazole po 500mg Q8hrs x 10-14 days • Treatment of moderate to severe disease (WBC > 15k or increasing cr) • Vancomycin po 125mg Q6hrs x 10-14 days
Clostridium difficile- Associated Disease • Treatment of severe disease (hypotension, obstruction, ileus, or perforation) • Metronidazole iv 500mg Q8hrs and vancomycin via NGT 500mg Q6hrs and/or vancomycin enema • Surgical consult • Consider colectomy if rising WBC and lactate
Clostridium difficile- Associated Disease • Recurrence • Occurs in 5-30% of patients • Rate does not vary with initial agent used • Can consider re-treatment with same agent • Consider vancomycin po pulse dosed (125-500mg Q 3days x 3 wks) or tapered • ? Role of cholestyramine and probiotics • ELISA not recommended as a test of cure in asymptomatic pts