Download
1 / 39
450 likes | 720 Views
Leading a High Reliability Organization. David Vaughan Executive Director Quality and Safety, Consultant Respiratory Paediatrician, Hamad Medical Corporation, Doha, Qatar. Disclosures. None, (But I have a lot of biases).

E N D
Leading a High Reliability Organization • David Vaughan • Executive Director Quality and Safety, • Consultant Respiratory Paediatrician, • Hamad Medical Corporation, • Doha, • Qatar
Disclosures • None, (But I have a lot of biases)
Leaders are visionaries with a poorly developed sense of fear and no concept of the odds against them Robert Jarvik
Learning Objectives • Understand that successful organizations coalesce around a simple message that everyone understands and can articulate • Be able to describe the features of HROs • Be able to describe how to measure a unit, team or organizational level of high reliability according to Weick and Sutcliffe framework • Be able to define how a HRO framework can assist healthcare in meeting many of the Berwick recommendations • Commit to applying the lessons learned on a small scale
Leadership behaviours that increase risk and make healthcare less safe: A promise to learn– a commitment to act. Improving the Safety of Patients in England. National Advisory Group on the Safety of Patients in England. P17
Have we improved? • “Sustained attention to patient safety has failed to produce widespread reductions in rates of harm.” • Trends in adverse events over time: why are we not improving? BMJ Qual Saf. 2013 Apr;22(4):273–7. Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010 Nov 25;363(22):2124–34.
Would you prefer to undergo complex surgery in.... • A hospital with a high rate of post-operative complications? • A hospital with a low rate of post-operative complications?
Patient safety problems exist throughout the NHS as with every other health care system in the world. NHS staff are not to blame – in the vast majority of cases it is the systems, procedures, conditions, environment and constraints they face that lead to patient safety problems. Incorrect priorities do damage: central focus must always be on patients. Warning signals abounded and were not heeded When responsibility is diffused, it is not clearly owned Improvement requires a system of support Fear is toxic to both safety and improvement.
I do not for a moment believe that those in responsible positions in the Trust went about their work knowing that by action or inaction they were contributing to or condoning the continuance of unsafe or poor care of patients. What is likely to be less comfortable is the possibility, and sometimes the likelihood, that whatever they believed at the time, they were not being sufficiently sensitive to signs of which they were aware with regard to their implications for patient safety and the delivery of fundamental standards of care. Unhappily, the word “hindsight” occurs at least 123 times in the transcript of the oral hearings of this Inquiry, and “benefit of hindsight” 378 times Francis Report, Volume 1
Normalisation of Deviance Once you have accepted an anomaly or something less than perfect, you have given up your virginity. You can’t go back. You’re at the point when it’s very hard to draw the line. Next time they say it’s the same problem, it’s just eroded 5 mm more. Once you accepted it, where do you draw the line? Once you have done it, it’s very difficult to go back now and get very hard nosed and say I’m not going to accept that” Diane Vaughan. The Challenger Launch Decision. University of Chicago Press. 1996
“There is no why here” “. . . I eyed a fine icicle outside the window, within hand’s reach. I opened the window and broke off the icicle but at once a large, heavy guard prowling outside brutally snatched it away from me. ‘Warum?’ I asked him in my poor German. ‘Hier ist kein warum’ (there is no why here), he replied, pushing me inside with a shove. Primo Levi
Why How What
Question In your organization, unit, department, can you outline the “Why” And if so, is it consistent across the organization? Is it simple & understood by everyone? If so, is it applied from the top down consistently?
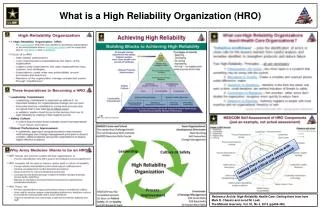
High Reliability Organisations HROs are organizations that function under very demanding conditions and manage to have fewer than their fair share of accidents
Mindfulness “To be mindful is to have a rich awareness of discriminatory detail and an enhanced ability to discover and correct errors that could escalate into a crisis” “When it comes to mindfulness, it’s good to feel bad, and bad to feel good”
HRO Features Preoccupation with failure Reluctance to simplify Resilience Mindfulness Sensitivity to operations Deference to expertise
Mindlessness When people function mindlessly, they don’t understand themselves or their environment, but they think they do They don’t know what they don’t know
“The situation in theatre appears to be fraught and the Panel learned of serious problems. It would appear that [the surgeon concerned] finds it difficult to work under stress, when the atmosphere becomes very tense. A number of theatre staff will not work with [X]. The Panel understand that there have been a number of complaints made against [X] and at least three of these were allegations of assault, which the Trust has investigated and dealt with accordingly ... when [X] is not in a stressful situation [X] is very charming and courteous when talking to patients ... [The surgeon] has no idea as to why there are these perceived problems;” Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry Volume 1: Ch 1 Warning Signs. P112
Pre-occupation with failure Failure implies something was not caught as soon as it could have been “At that stage, therefore, neither SaSSHA nor the DH, up to ministerial level, can have been in any doubt that there were potentially serious managerial issues, particularly in relation to finance, and record systems, at the Trust and that close supervision of its performance was Necessary” Francis Report. Volume 1. P60
Pre-occupation with Failure Audit What surprised you? How would a front line worker answer? How frequently do you consider what might go wrong?
Reluctance to Simplify Seek divergence in viewpoints; multiple views, especially from the front line. The report was extremely damaging, more than justifying the complaints that had been made. The report noted that: Ward 3 is known by reputation to have had long-standing problems (many years) in standards of patient care which are generally put down to the heavy workload and poor staffing. Francis Report. Vol 1. P64
Reluctance to Simplify Can you recall a serious safety event that with hindsight was due to an inappropriate simplification?
Sensitivity to Operations Being aware of current operational work enables organisations to catch small errors and mistakes which almost always manifest first at the front line “we’re sinking under patients in A&E. Any support would be gratefully received. We’ve tried to get hold of the Community matrons but only got a voicemail service. We have 12 ambulances queuing” Francis Report. Vol 1. P98
Sensitivity to Operations Outline an example where increased awareness of front line operations in your area of responsibility might reduce the risk of failure
Commitment to Resilience How well prepared are we to manage the unexpected when it does happen? “The Board was made aware of the 2006 survey figures at the meeting on 3 May 2007 when it was reported that the Trust was in the worst 20%. Predictably, an action plan was said to have been developed.” Francis Report. Vol. 1. P
Questions What is your worst fear? How well prepared are you to handle if this became reality?
Questions • Can you identify the following characteristics on the video shown? • Pre-occupation with failure • Reluctance to simplify • Sensitivity to operations • Commitment to resilience
Deference to Expertise HROs shift their work in moments of crisis to those best placed to understand the work “A clear deficit” in trained emergency medicine consultants and the department was not covered 24/7 by an accredited emergency department consultant. The report was greeted with a somewhat laconic response by Dr Moss, who, in circulating it to colleagues said:“Suggest we all have a read and if there are any burning problems identified please can you let me know” Francis Report. Vol 1. Warning Signs. P130
Muething SE, Goudie A, Schoettker PJ, Donnelly LF, Goodfriend MA, Bracke TM, et al. Quality Improvement Initiative to Reduce Serious Safety Events and Improve Patient Safety Culture. PEDIATRICS. 2012 Aug 1;130(2):e423–31.
Leadership behaviours that increase risk and make healthcare less safe: • Make bad news unwelcome (too often silencing it) • Blame staff (even when they haven’t been given the conditions for success • Not heed signals and warnings that things are amiss • Fail to listen to staff • Diffuse responsibility and disguise who is in charge • Lead by rules and procedures alone in a disengaged way • Apply sanctions to errors • Fail to focus on the patient (often signalling instead that targets and costs are ‘centre stage’) • Muffle the voice of the patients, their carers and their families and largely ignore their complaints • Offer no systematic support for improvement capability • Game data and goals • Create fearfulness amongst colleagues and staff • Ignore the development of the next generation of leaders • Treat all problems as though they can be “fixed” with existing technologies or writing clearer procedures A promise to learn– a commitment to act. Improving the Safety of Patients in England. National Advisory Group on the Safety of Patients in England. P17
Leadership behaviours that increase risk and make healthcare less safe: A promise to learn– a commitment to act. Improving the Safety of Patients in England. National Advisory Group on the Safety of Patients in England. P17
Next Steps • Consider using these audits on your unit, department • Walk the walk • Increase the number of mindful moments in your unit • Identify a modest problem, look at failures, assume nothing, develop a solution and focus on the expert in handling the problem rather than blaming the person “responsible”