Download
1 / 13
130 likes | 279 Views
COPD Update Chronic Obstructive Pulmonary Disease. David Henke MD, MPH. N Engl J Med 356;8 Feb. 2007. Dynamic Narrowing. Kurosawa, H. et al. N Engl J Med 2004;350:1036. Diagnosis of COPD. Symptoms Cough Sputum Dyspnea. Exposure to risk factors Tobacco smoke Occupation

E N D
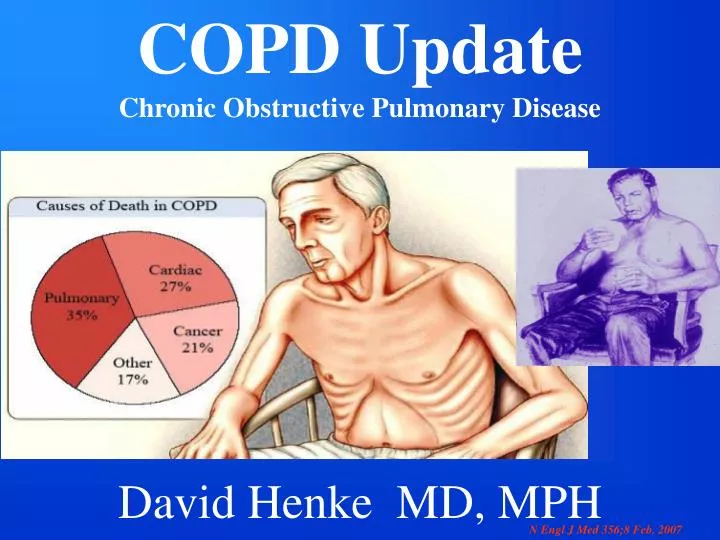
COPD Update Chronic Obstructive Pulmonary Disease David Henke MD, MPH N Engl J Med 356;8 Feb. 2007
Dynamic Narrowing Kurosawa, H. et al. N Engl J Med 2004;350:1036
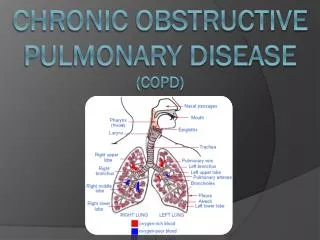
Diagnosis of COPD Symptoms Cough Sputum Dyspnea Exposure to risk factors Tobacco smoke Occupation Indoor/outdoor pollution Spirometry GOLD Guidelines, 2001.
What Happens To Smokers? Doll-BMJ. 2004 June 26;328(7455):1519 • 50% of Persistent Smokers Killed By Their Habit - 25% age 35-69 • Full Impact On National Mortality Takes > 50 Years To Realize • Smoking Doubles Age Specific Mortality In Middle & Old Age • Longevity Has Improved Rapidly But Not For Smokers • Stopping At 50 Y.O. Halved The Hazard • Stopping At 30 Y.0. Avoided Most Of the Risk • Smokers Die About 10 YRS. Younger
Towards a Revolution in COPD Health (TORCH) • Combination ICS & Long-acting Beta agonists (LABA) outcome: 18% reduction of all-cause death over 3yrs. Intention to Rx: 39 pts to save 1 life over 3yrs. P=0.052 • Mono-therapy ICS associated with more pneumonia • No adverse risk with LABA therapy (not powered for African Americans) • Combination Therapy verses either mono-therapy: • Better health status • Fewer exacerbations-- • Less oral steroids • Protection against declining lung function (Similar results AJRCCM 175 Jan. 2007) NEJM 356;8,2007
Clinic Patient • 65 y.o. white female (60p/y smoker)w/o sx’s . Concerned about smoking, husband insisted she see MD. • Performs ADLs, worked as hostess in son’s restaurant • NoSOB/DOE. • Mildly obese/ normal physical
What Do I Tell My Patient With A Concerned Husband Who Denies Symptoms? • I Don’t Care If You Have COPD Because You Smoke And If You Have It You Deserve It • I’ll Give You A Valium Prescription So You Can Sedate Your Hyper-Vigilant Husband • You May Have COPD Because You Smoke Even Though You’re Not Aware Of Symptoms. The Only Way To Be Sure Is To PerformSpirometry.
65 y.o. white female (60p/y smoker)w/o sx’s Spirometry DLCO 13.5 ml/mmHg/min. %Ref 63% ABG (RA): pH 7.42 CO2= 41 O2=66 After Bronchodilator CXR: Hyperinflation % Ref TLC 120% FRC (pl) 137% RV 169% Pre % RefPost % Ref9 months later FVC79%83%(5%) 93% FEV151%57%(12%) 67% FEV1/FVC 49%53%55% 25-75%16%30%(92%) 32% PEFR L/sec3.67 3.97home 2.104.57home 3.75
Progressive Dyspnea In COPD 86 y.o. male with 90 py smoking D/Ced 1968 with worsening: CRI (Cr.4.7), chronic diarrhea (?etiology), HTN, s/p CVA, s/p biliary stent. CC: 7months of progressive DOE; new supplemental O2 need HPI: Still active and into his business office daily without dyspnea until 7 mos. PTA developed SOB walking from the car to office. Patient now wheelchair dependent and unable to work. Page 1/3: case 84084-3
Pulmonary Function Test Case Spirometry: (PRE) (POST) FVC 4.15 (101%) 4.37 (106%) FEV1 2.47 (86%) 2.73 (95%) FEF25-75 0.93 (50%) 1.54 (82%) 6 min. walk: Sats 80’s% ABG/RA: pH 7.39 PaO2: 58 mmHg PaCO2: 23 mmHg Diffusion: DLCO ml/mmHg/min: 8.1 (35%) DLCO/Va ml/mmHg/min: 1.51 (45%) Page 2/3: case 84084-3
High Probability VQ For Pulmonary Embolus Most COPD pts die from extra- pulmonary dz, e.g., 25% of severe exacerbations w/o clear cause & resulting in hospitalizations had PEs. (Ann Intern Med. 2006;144:390) Page 3/3: case 84084-3
Summary • Relay on Risk & Spirometry(symptoms) to dx COPD • Therapeutic cornerstone in smokers with COPD: • Smoking Cessation • Only smoking cessation and maintaining • Hgb sats. > 90% prolong life • Early detection & Rx for COPD can preserve & improve lung function (Combination vs ICS or B-agonist mono-RX: may be the more effective) • Most COPD patients die from non-pulmonary dz