Download

1 / 15
150 likes | 350 Views
Diagnosing Asthma in Adults. What is asthma ? -a chronic inflammatory disorder of the airways -associated with airway hyper-responsiveness - leading to recurrent episodes of wheezing , breathlessness , chest tightness and coughing particularly at night or in the early morning.

E N D
What is asthma ? -a chronic inflammatory disorder of the airways -associated with airway hyper-responsiveness -leading to recurrent episodes of wheezing, breathlessness, chest tightness and coughing particularly at night or in the early morning. • episodes are usually associated with widespread but variable airflow obstruction within the lung that is often reversible either spontaneously or with treatment (GINA)
or more simply .. -asthma is a condition of paroxysmal reversible airway obstruction which is characterised by : • Airflow limitation ( reversible) • Airway hyper- responsiveness • Inflammation of the bronchi
UK, 5.4 million people currently receiving treatment for asthma • 1.1 million of whom are children • 25% adults 20-44yrs suffer with wheeze • 15% suffer from wheeze with breathlessness
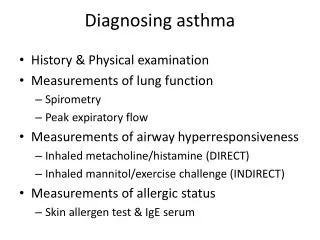
Diagnosing Asthma • Genetic / environmental influence • Based on : -History : pattern of symptoms ?Exposure to tobacco/cats/exercise worsen sx -Exam : Nasal polyps/expiratory wheeze -spirometry/PEF -response to therapy
Symptoms indicating high probabIlity of asthma • More than one of the following symptoms: wheeze, breathlessness, chest tightness and cough • particularly if: • symptoms worse at night and in the early morning • symptoms in response to exercise • allergen exposure and cold air • symptoms after taking aspirin or beta blockers • History of atopic disorder • Family history of asthma and/or atopic disorder • Widespread wheeze heard on auscultation of the chest • Otherwise unexplained low FEV1 or PEF (historical or serial readings) • Otherwise unexplained peripheral blood eosinophilia
Symptoms that lower probabilIty of asthma -Prominent dizziness -light-headedness -peripheral tingling -Chronic productive cough in the absence of wheeze or breathlessness -Repeatedly normal physical examination of chest when symptomatic -Voice disturbance -Symptoms with colds only -Significant smoking history (ie > 20 pack-years) -Cardiac disease • Normal PEF or spirometry when symptomatic A normal spirogram/spirometry when not symptomatic does not exclude the diagnosis of asthma. Repeated measurements of lung function are often more informative than a single assessment.
Spirometry • CXR/bloods • FEV1= forced expiratory volume in 1 minute (reduced in restrictive and obstructive disease) • FVC = forced vital capacity (Reduced in restrictive disease and obstructive disease) • FEV1/FVC = normal in restrictive, reduced in obstructive disease • FEV1/FVC <70% = obstructive disease -confirm reversibility of airflow obstruction -defined by improvement in FEV1 by > 12% and 400mls by the use of a short acting bronchodilator or a course of prednisolone (30mg od for 2/52)
pef • PEF showing diurnal variability -highest daily PEFR-Lowest daily PEFR/(highest daily PEFR) • diagnosis of asthma is supported if PEFR varies by at least 20% for 3 days in a week over several weeks or PEFR increases by at least 20% in response to asthma treatment. • Nb : doesn’t reflect the level of lung obstruction as well as lung function testing
Suspected Asthma Clinical assessment + Spirometry (or PEF if spirometry not available) • High probablity Intermediate probablity low probablity TREAT FEV1/FVC<0.7 FEV1/FVC>0.7 treat other condition and assess response ? Further IX Further assessment and referral
Referral criteria • diagnosis unclear • unexpected clinical findings (ie crackles, clubbing, cyanosis, cardiac disease) • unexplained restrictive spirometry • suspected occupational asthma • persistent non-variable breathlessness • monophonic wheeze or stridor • prominent systemic features (myalgia, fever, weight loss) • chronic sputum production • CXR shadowing • marked blood eosinophilia (>1 x 10^9/l) • poor response to asthma treatment • severe asthma exacerbation
Classification severity of asthma • Mild intermittent: Symptoms ≤2 times a week Asymptomatic and normal peak expiratory flow rate (PEFR) between attacks Attacks are brief with varying intensity Night-time symptoms ≤2 times a month Forced expiratory flow at 1 second (FEV1) or PEFR ≥80% of predicted PEFR variability <20%. • Mild persistent: Symptoms >2 times a week but <1 time a day Exacerbations may affect activity Night-time symptoms >2 times a month FEV1 ≥80% of predicted PEFR variability between 20% and 30%
Moderate persistent: Daily symptoms Use of short-acting beta agonists daily Attacks affect activity Exacerbations ≥2 times a week and may last for days Night-time symptoms >1 time a week FEV1 greater than 60% to <80% of predicted PEFR variability >30%. • Severe persistent: Continual symptoms Limited physical activity Frequent exacerbations Frequent night-time symptoms FEV1 ≤60% of predicted PEFR variability >60%.
What about COPD ? • COPD = generally >35yrs • Risk factor =smoker, regular sputum production • No diurnal variation in symptoms, very little variability in PEFR • FEVI<70%, FEV1/FVC<0.7 • <15% response to reversibility test • Single breath diffusing capacity (Lung function tests) • Normal person DLC0 75-125%, Reduced in COPD
References • Nice guidelines • BTS/Sign guidelines • Oxford handbook GP