Download
1 / 1
10 likes | 119 Views
No. 179. Patients' and their doctors’ preferences for adjuvant sorafenib after resection of intermediate to high risk RCC: what makes it worthwhile?.

E N D
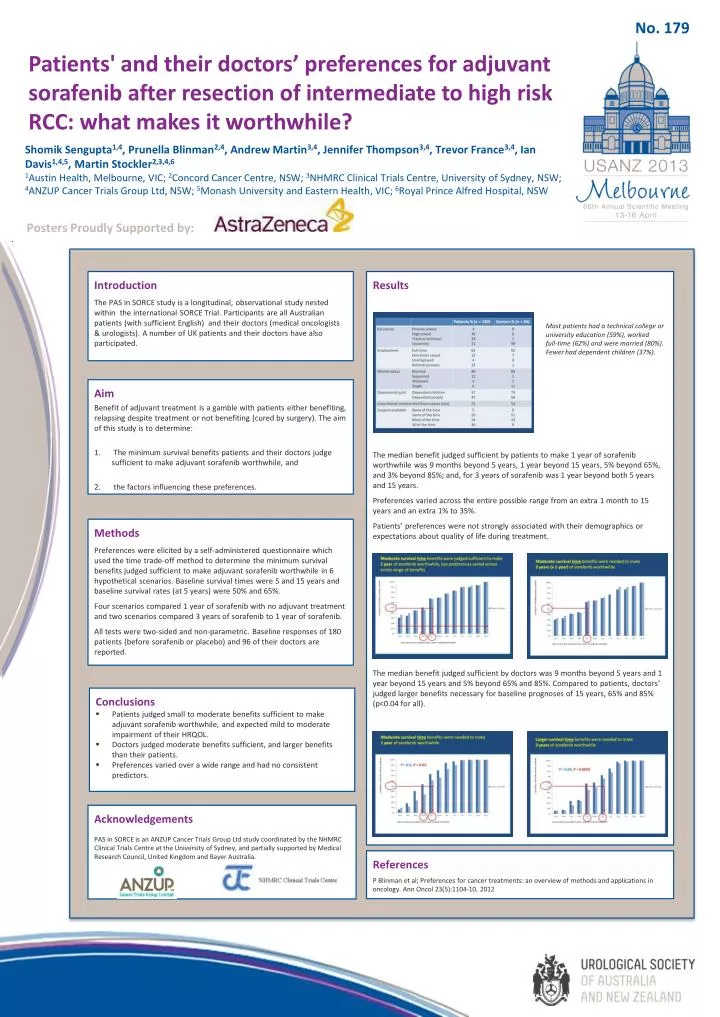
No. 179 Patients' and their doctors’ preferences for adjuvant sorafenib after resection of intermediate to high risk RCC: what makes it worthwhile? Shomik Sengupta1,4, Prunella Blinman2,4, Andrew Martin3,4, Jennifer Thompson3,4, Trevor France3,4, Ian Davis1,4,5, Martin Stockler2,3,4,6 1Austin Health, Melbourne, VIC; 2Concord Cancer Centre, NSW; 3NHMRC Clinical Trials Centre, University of Sydney, NSW; 4ANZUP Cancer Trials Group Ltd, NSW; 5Monash University and Eastern Health, VIC; 6Royal Prince Alfred Hospital, NSW Posters Proudly Supported by: Results The median benefit judged sufficient by patients to make 1 year of sorafenib worthwhile was 9 months beyond 5 years, 1 year beyond 15 years, 5% beyond 65%, and 3% beyond 85%; and, for 3 years of sorafenib was 1 year beyond both 5 years and 15 years. Preferences varied across the entire possible range from an extra 1 month to 15 years and an extra 1% to 35%. Patients’ preferences were not strongly associated with their demographics or expectations about quality of life during treatment. The median benefit judged sufficient by doctors was 9 months beyond 5 years and 1 year beyond 15 years and 5% beyond 65% and 85%. Compared to patients, doctors’ judged larger benefits necessary for baseline prognoses of 15 years, 65% and 85% (p<0.04 for all). Introduction The PAS in SORCE study is a longitudinal, observational study nested within the international SORCE Trial. Participants are all Australian patients (with sufficient English) and their doctors (medical oncologists & urologists). A number of UK patients and their doctors have also participated. Most patients had a technical college or university education (59%), worked full-time (62%) and were married (80%). Fewer had dependent children (37%). Aim Benefit of adjuvant treatment is a gamble with patients either benefiting, relapsing despite treatment or not benefiting (cured by surgery). The aim of this study is to determine: The minimum survival benefits patients and their doctors judge sufficient to make adjuvant sorafenib worthwhile, and the factors influencing these preferences. Methods Preferences were elicited by a self-administered questionnaire which used the time trade-off method to determine the minimum survival benefits judged sufficient to make adjuvant sorafenib worthwhile in 6 hypothetical scenarios. Baseline survival times were 5 and 15 years and baseline survival rates (at 5 years) were 50% and 65%. Four scenarios compared 1 year of sorafenib with no adjuvant treatment and two scenarios compared 3 years of sorafenib to 1 year of sorafenib. All tests were two-sided and non-parametric. Baseline responses of 180 patients (before sorafenib or placebo) and 96 of their doctors are reported. • Conclusions • Patients judged small to moderate benefits sufficient to make adjuvant sorafenib worthwhile, and expected mild to moderate impairment of their HRQOL. • Doctors judged moderate benefits sufficient, and larger benefits than their patients. • Preferences varied over a wide range and had no consistent predictors. Acknowledgements PAS in SORCE is an ANZUP Cancer Trials Group Ltd study coordinated by the NHMRC Clinical Trials Centre at the University of Sydney, and partially supported by Medical Research Council, United Kingdom and Bayer Australia. References P Blinman et al; Preferences for cancer treatments: an overview of methods and applications in oncology. Ann Oncol 23(5):1104-10, 2012






