Download
1 / 60
1.32k likes | 4.75k Views
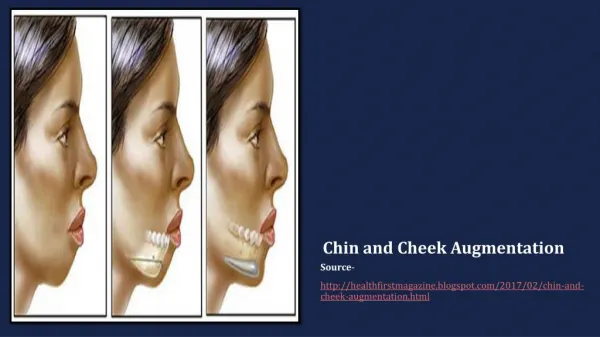
Facemask and Chin cup. Dr Abdul Jabbar. What are facemasks and chin cups? . Growth modification appliances for skeletal Class III. CLASS III MALOCCLUSION. The relative mesiodistal relation ship of arches are abnormal with all the lower teeth occluding mesial to

E N D
Facemask and Chin cup Dr Abdul Jabbar
What are facemasks and chin cups? • Growth modification appliances for skeletal Class III.
CLASS III MALOCCLUSION • The relative mesiodistal • relation ship of arches are • abnormal with all the lower • teeth occluding mesial to • normal ,producing marked • disharmony in the incisor • region and in the facial lines.
CLASS III MOLAR RELATION SHIP Abnormal relationship in which the mesiobuccal cusp of max. first permanent molar occludes distal to the buccal groove of mandibular first molar.
TYPES OF CLASS III MALOCCLUSION DENTAL FUNCTIONAL SKELETAL Short Maxilla Prognathic Mandible Composite
Dental Class III • Early loss of lower e`s
DENTOALVEOLAR MAL-RELATIONSHIP FEATURES • No apparent saggital discrepancy • ANB angle is with in normal limits • Lingual tipping of max. incisors & labial tipping of mand. incisors
ETIOLOGICAL FACTORS FUNCTIONAL (PSEUDO) CLASS III MALOCCLUSION
Dentalfactors • Ectopic eruption of maxillary central incisors • Premature Contact • Premature loss of C`s
Functional factors • Anomalies in tongue position • Neuromuscular features • Naso-respiratoryor airway problems
Skeletal Factor • Minor transverse maxillary discrepancy
FEATURES OF PSEUDO CLASS III • Mandible appear morphologically normal • Class I or mild Classlll sk. Relationship • Ant. cross bite and negative over jet is present due to a ant Displacement of mandible • Mandible can be pushed back to edge-edge relationship
1. GROWTH MODIFICATION Pre Adolescents (late childhood , juvenile) Adolescents (v. minimal effects) 2. CAMOFLOUGE (MILD) Adolescents Adults 3. Orthognathic SURGERY (moderate –severe) Post adolescents Adults
GROWTH MODIFICATION • SK CLASS III CAUSES DEFICIENT MAXILLA PROGNATHIC MANDIBLE COMPOSITE
FACE MASK THERAPY • Orthopedic face mask correct classIII malocclusion in: • Late decidious or early permenant dentition • Changes produced in all three plane of spaces
TREATMENT EFFECTS PRODUCED BY FACE MASK THERAPY • Correction of CO_CR discrepancy • Maxillary sk. Protraction • Forward movement of max.dentition • Lingual tipping of lower incisors • Redirection of mand. Growth in more vertical direction
TREATMENT IN GROWING PATIENTS(pre- adolescents , adolescents) • Skeletal Class III with • Short Maxilla • FR 3 (22-23 hrs) • Effects • Forward mov.of maxilla • Proclination of upper incisors • Backward rotation or repositioning of mand. • Increase in lower ant. Facial height • lingual tipping of lower incisors
TREATMENT IN GROWING PATIENTS(pre adolescents , adolescents) • Composite Skeletal Class III • -ive Family History • Face Mask or Reverse Headgear Pre-requisite Maxillary Expansion • Effects • Maxillary sk. Protraction • Forward movement of max.dentition • Lingual tipping of lower incisors • Redirection of mand. Growth in more vertical direction
Treatment effects • Incease in overjet (4.4 mm)Mesial mov. &flaring of upper incisors & up righting of lower incisors • & correction of molar position towards class I molar correction(3.1 mm)mesial mov. Of maxilla • Skeletal effects • ANB angle (2.4-2.8)& Witts appraisal(witts value 2.6mm)
Treatment & Managementin Pre-adolescence DEFICIENT MAXILLA/COMPOSITE III Expansion + face mask • 8 yrs ideal age for maxillary protraction. • more the age of the patient ,less will be the skeletal effects. • early ages treatment ensures better skeletal effects.
Criterea for facemask: • Short face Normal face • Lower incisors either normally inclined or proclined. • Upper incisors must be either retroclined or normally inclined. • Growing 8yrs age ideal for facemask
Components of orthopedic facial mask therapy • Facial mask • Bonded max. expansion splint • Heavy elastics
FACE MASK THERAPY • Orthopedic face correct classIII malocclusion in • Late decidious or early permenant dentition • Changes produced in all three plane of spaces
Facial mask • Facemask therapy often follows maxillary expansion since the latter disrupts the circummaxillarysutural system and facilitates the orthopedic effects of the facemask • children treated at an early age, showed a significant forward displacement of the maxillary complex and a significant upward and forward direction of condylar growth, leading to smaller increments in total mandibular length
Types of facemasks • Delaire facemask 2. Petit facemask
Facial mask • made of two pads that contact the soft tissue in the forehead and chin regions.. • The pads are connected by a rod • In the center of the midline framework is adjustable crossbow to which elastics are connected bilaterally
2 .Max.expansionsplint • The second component of this orthopedic treatment is the maxillary splint. an acrylic and wire maxillary expansion appliance that is bonded to the posterior dentition. • In mixed dentition cases, the splint usually covers the first and second deciduous molars. • The upper canines may also be included in patients who present with complete deciduous dentitions.
Max.expansion splint • maxillary splint is made of a framework of .045“(1.2mm) round stainless steel wire, to which an expansion screw is attached. • If second molars are present, an occlusal rest is extended to the second molars to prevent overeruption of these teeth during treatment (Two hooks, to which elastics are attached, are soldered to the wire framework. • These hooks usually lie adjacent to the canines or first deciduoud molars.
Max.expansion splint • , Rapid palatal expansion can produce a slight forward movement of Point A and a slightdownward and forward movement of the maxilla. • In the context of facial mask therapy, the effect of such expansion is to disrupt the maxillary sutural system, thus possibly enhancing the effect of the orthopedic facial mask by making sutural adjustments occur more readily.
Another advantage of maxillary expansion is the correction of the posterior crossbite that often accompanies a Class III malocclusion because of deficient transverse maxillary growth and the abnormal anteroposterior relationship of maxilla to mandible. • In addition, a palatal expansion appliance splints the maxillary dentition during protraction and helps transmit force from the teeth to the maxilla, thus limiting unwanted tooth movement.
Activation of splint • The patient is usually instructed to turn the midline jackscrew of the appliance once daily, generally before bedtime. • In the majority of Class III individuals in whom use of an orthopedic facial mask is indicated, some maxillary expansion is beneficial. In such a case, the maxillary splint is expanded until the desired transverse change is achieved.
Activation of splint • In instances in which no transverse change is necessary, the maxillary splint is activated once a day for eight days to produce a disruption in the sutural system that facilitates the action of the facial mask
Heavy elastics • The facial mask is secured to the face by stretching elastics from the hooks on the maxillary splint to the crossbow of the facial mask • Heavy forces are generated, usually through the use of 5/16", 14oz elastics bilaterally. • Lighter forces may be used during the break-in period, but forces should be increased as the patient adjusts to the appliance.
INSTRUCTIONS • Optimally, the patient is instructed to wear the facial mask on a full-time basis except during meals. • Young patients (5 to 9 years old) can usually follow this regimen, particularly if the patient is told that the full-time wear will last only three to five months. • In older patients, full-time wear may not be possible, in which case the appliance should be worn at all times except when the patient is in school or participating in contact sports
FACIAL MASK The facial mask is usually worn until a positive overjet of 2-4mm is achieved interincisally. At this time, part-time or nighttime wear is recommended for an additional three to-six-month retention FR-3 Frankel appliance1 can be worn as an active retainer.
Skeletal classIII with large mandible • Extra oral force application can be accomplished in 2 ways: • EO force through condyles • EO force below the condyles.
What appliance? Chin cup Types of chin cup
SKELATAL CLASS III WITH LARGE MANDIBLE • Pre adolescents, mild, no family history, low angle Chin Cup • Adolescents ,mild Class III ,low angle. Chin Cup or surgical preparation. • Adults Camoflouge of surgery
growth philosophy • Mandibular growth mechanisms • functional matrix theory • displacements primary and s secondary. 3. Growth sites and growth centers. 4. Drift , relocation, sub periosteal deposition and resorption, modelling,remodelling.
TREATMENT IN GROWING PATIENTS Skeletal Class III with PrognathicMandible -iveFamily History Reverse Twin Block ( appliances without lip pads) Chin Cup 1. Occipital Pull 2. Vertical Pull 150-300 gm per side (INITIALLY) 450-700 gm (if force is directed through condyle & slightly less if below the condyle) 14 hrs per day After correction of cross bite wear only at night as retention appliance
Chin cup types CHIN CUP TYPE HEAD GEAR 2.VERTICAL PULLCHIN CUP 1.OCCIPITAL- PULL CHIN CUP
OCCIPITAL- PULL CHIN CUP • Mild to moderate mand. Prognathism • Short lower ant. Facial hgt. • Normally positioned or slightly proclined lower incisors(some backward tipping of lower incisors)