Download
1 / 44
490 likes | 850 Views
Hepatic Failure-1,2. By Dr. A bdelaty S hawky Assistant Professor of Pathology. Introduction.

E N D
Hepatic Failure-1,2 By Dr. Abdelaty Shawky Assistant Professor of Pathology
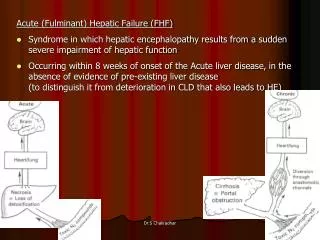
Introduction • The most severe clinical consequence of liver disease is hepatic failure. This may be the result of sudden and massive hepatic destruction or it is the end point of progressive damage to the liver as part of chronic liver disease. • Whatever the cause, 80% to 90% of hepatic functional capacity must be eroded before hepatic failure ensues.
In most cases of severe hepatic dysfunction, liver transplantation is the only hope for survival.
* The causes of hepatic failure fall into three categories: 1. Massive hepatic necrosis: due to; • Drug-induced, as from acetaminophen, halothane, antituberculosis drugs (rifampin, isoniazid), antidepressant monoamine oxidase inhibitors. b. Hepatitis: Hepatitis A infection accounts for 4% of cases, hepatitis B infection accounts for 8%. Hepatitis C infection does not cause massive hepatic necrosis.
2. Chronic liver disease: This is the most common route to hepatic failure and is the endpoint of progressive chronic hepatitis ending in cirrhosis. 3. Hepatic dysfunction without overt necrosis: Hepatocytes may be viable but unable to perform normal metabolic function, as with Reye syndrome and acute fatty liver of pregnancy.
Reye's syndrome • Is a potentially fatal disease that has numerous serious effects to many organs, especially the brain and liver. • The classic features are a rash, vomiting, and liver damage. • The exact cause is unknown and, while it has been associated with aspirin consumption by children with viral illness, it also occurs in the absence of aspirin use. • The disease causes fatty liver with minimal inflammation and severe encephalopathy (with swelling of the brain). • Jaundice is not usually present. • Early diagnosis is vital; although most children recover with supportive therapy, it may lead to severe brain injury and death.
Topics: • Liver necrosis. • Hepatitis. • Cirrhosis. • Portal hypertension. • Hepatic tumors. • Manifestations of Hepatic failure. • Hepatorenal syndrome. • Laboratory evaluation of liver diseases. • Clinical cases.
A. Necrosis with intact liver framework 1. Apoptosis (Necrobiosis): * Def. death of single scattered hepatocytes. * Causes: 1. Acute viral hepatitis 2. Yellow fever. * N/E: No gross abnormalities. * M/P: the cytoplasm is deeply acidophilic and the nucleus becomes pyknotic. When the nucleus disappears, councilman body is produced. * Clinical features: No jaundice. * Fate: regeneration is complete.
2. Piece meal necrosis: * Def. apoptosis of peripheral hepatocytes resulting in moth eaten appearance of the limiting plates. * Causes: 1. Chronic hepatitis. 2. Submassive hepatic necrosis. * N/E: No gross abnormalities. * M/P: irregular moth eaten limiting plate. * Clinical features: No jaundice. * Fate: regeneration is complete.
3. Focal (spotty) necrosis: * Def. necrosis of small groups of hepatocytes. * Causes: 1. Acute viral hepatitis. 2. Severe toxemia & anemia. * N/E: scattered yellow (necrotic) foci. * M/P: necrotic small groups of hepatocytes surrounded by macrophages & lymphocytes. * Clinical features: No jaundice. * Fate: regeneration is complete.
4. Bridging (confluent) necrosis: * Def. wide areas of necrosis associated with collapsed reticulin framework extends from a lobule to the other. May be portal-portal bridging necrosis or portal-central bridging necrosis or central-central bridging necrosis. * Causes: • Chronic hepatitis with submassive hepatic necrosis. • Shock. • Toxemia of pregnancy. • Alcoholism. * N/E: minute yellow dots & streaks.
* Clinical features: jaundice. * Fate: regeneration is complete. * Complications: fulminant hepatic failure may occur.
B. Necrosis with destroyed liver framework: • Necrosis of hepatocytes associated with destruction of the reticulin framework of the liver. * Include; Panacinar necrosis * Causes: • Acute viral hepatitis. • Hepatotoxic agents: halothane, paracetamol, carbon tetrachloride. * Pathology: wide areas of yellowish necrotic patches range from submassiveto massive necrosis
* Etiology:HAV, HBV, HCV, HDV, HEV. * Pathogenesis: Liver cell injury is caused by: • Direct cytopathic effect of the virus. • Cell mediated immune response (by cytotoxic T lymphocytes).
* Clinical course:4 stages; a. I.P “incubation period”. b. Pre-icteric phase: non-specific constitutional symptoms (serum sickness-like syndrome, urticaria, skin rash, arthritis & glomerulonephritis). c. Icteric phase: jaundice, dark urine, light colored stool & pruritis. d. Convalescence stage: for few weeks.
* Pathology: • Two forms; a. Typical (classic) acute viral hepatitis with focal necrosis. b. Acute viral hepatitis with Panacinar necrosis (fulminant viral hepatitis).
* Definition:chronic inflammatory liver disease. * Etiology: 1. Viral: HBV (+/_ HDV), HCV or mixed. 2. Autoimmune: due to auto-antibodies as antinuclear, anti-mitochondrial antibodies…. 3. Drug induced: INH, methyl dopa. 4. Metabolic: congenital α1 anti-trypsin deficiency, Wilson disease. 5. Cryptogenic: idiopathic.
* Clinical course:unpredictable, the patient may show spontaneous remission, or have an indolent course or may show progressive liver cell failure. * N/E: mild hepatomegally.
* M/P: - include the following features; I. Portal tracts show: a. Piece meal necrosis: necrosis of the hepatocytes at the limiting plate. b. Portal tract inflammation: • Chronic inflammatory cells; lymphocytes, macrophages with occasional plasma cells. • Lymphoid follicle formation (with HCV). • Bile duct inflammation (with HCV).
II. The hepatic lobules show: • Degeneration: Fatty change (with HCV). • Necrosis: • Focal (spotty) necrosis surrounded by chronic inflammatory cells. • Confluent necrosis and bridging necrosis: with progressive hepatitis. • Dysplasia of hepatocytes (precancerous). • Von Kupffer cell hyperplasia.
Specific diagnostic lesions: • Ground glass appearance of hepatocytes (with HBV). • Presence of PAS +ve globules inside the hepatocytes (with congenital α1 antitrypsin deficiency). • Presence of cupper particles inside the hepatocytes (with Wilson disease). • Rosseting: occasional arrangement of a group of hepatocytes around a central bile canaliculus. Characteristic of auto-immune hepatitis.
The periportal red hyaline globules seen here with periodic acid-Schiff (PAS) stain are characteristic for alpha-1-antitrypsin (AAT) deficiency.
III. Fibrosis & Cirrhosis:Periportal fibrosis or bridging fibrosis leads finally to mixed (micro and macronodular) or macronodular cirrhosis. Macronodular cirrhosis is precancerous.
* Grading of chronic hepatitis by assessment the degree of activity: • This is done by examining 4 parameters; portal inflammation, piece meal necrosis, focal (spotty) necrosis and confluent necrosis. The degree of activity is graded as mild, moderate and marked according to the score of these parameters.
* Staging of chronic hepatitis: • By assessment of the degree of fibrosis
* Complications of chronic hepatitis: • Post-hepatitic cirrhosis. • Liver cell failure. • Hepatocelluar carcinoma.