Download
1 / 13
130 likes | 139 Views
NATURAL HISTORY OF BETA CELL FAILURE IN T2DM. BUT We ’ ve been taught: ‘ Beta cell failure occurs much earlier in the natural history of type 2 diabetes and is more severe than previously appreciated ’ Helps ‘ confirm ’ impression that most T2DM patients will need insulin.

E N D
NATURAL HISTORY OF BETA CELL FAILURE IN T2DM BUT We’ve been taught: ‘Beta cell failure occurs much earlier in the natural history of type 2 diabetes and is more severe than previously appreciated’ Helps ‘confirm’ impression that most T2DM patients will need insulin
Belfast Diet Study-Bi-phasic Loss of B-Cell FUNCTION My Translation- Glucotoxicity 2% /yr decline 18%/yr decline DX DM Deteriorating beta-cell function in type 2 diabetes: a long-term model. Bagust A, Beale S. QJM. 2003 Apr;96(4):281-8
UKPDS: Patients Requiring InsulinOver the Course of Their Diabetes 60 Chlorpropamide Glipizide 40 Patients Requiring Additional Insulin (%) 20 0 1 2 3 4 5 6 Years from Randomization But remember, SU’s cause Beta-Cell APOPTOSIS Adapted from: Wright A, et al. Diabetes Care. 2002;25:330–336.
But even after 15 years of DM, MOST have >40% of beta cell mass
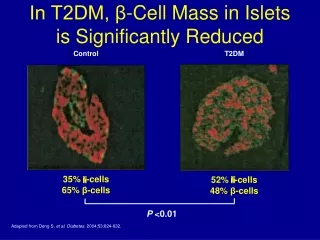
Beta-Cell Mass Reduced, but most have > 20% nml; Non-DM DM J. Rahier , Diabetes, Obesity, Metab 10 2008: 32-42
We’ve been taught DM is progressive Lose of 50% of function by Dx Type 2 Diabetes Is Progressive
CV Risk of SU and InsulinIn ‘Real World Use’ So benefit of both SU/Insulin in research studies –UKPDS, DCCT/EDIC But adverse risk in ‘real world’ use- would not pass current FDAguidelines for CV risk with a new agent Pharmacoepidemiology and Drug Safety. 2008;(17):753-759.
Value to Early Insulin Therapy-Outweighed By Hypoglycemia Weight GainEspecially when one can reduce lipotoxicity and Glucotoxicy , just as fast, with new anti-hyperglycemic agents
Initial Triple Combination Therapy is Superior to ADA Guideline Triple Therapy subjects had a 13.6-fold lower rate of hypoglycemia compared to subjects receiving Conventional Therapy. Triple Therapy subjects had mean weight loss of 1.2 kg versus 3.6 kg weight gain (p=0.02) in subjects on Conventional Therapy. Diabetes Obes Metab. 2014 Nov 26. doi: 10.1111/dom.12417. [Epub ahead of print] Initial combination therapy with metformin, pioglitazone and exenatide is more effective than sequential add-on therapy in subjects with new-onset diabetes. Results from the Efficacy and Durability of Initial Combination Therapy for Type 2 Diabetes (EDICT): a randomized trial. Abdul-Ghani MA1, Puckett C, Triplitt C, Maggs D, Adams J, Cersosimo E, DeFronzo RA
Some Small Number WILL need Basal Insulin Diabetes Disease Progression An Alternative Approach Start BASAL insulin Include Incretin Start 1-3 non-insulin Therapy(ies) Diet/exercise DPP-4, dipeptidyl peptidase-4; GLP-1R, glucagon-like peptide-1 receptor. Rodbard HW et al. Endocrine Pract. 2009;15:540-559. Available at: http://www.aace.com/pub/pdf/GlycemicControlAlgorithmPPT.pdf. December 2009 update.
Issues 1. Tells you CONSIDER stopping SU- MUST 2. Doesn’t tell you what to do with other non-insulin therapies-CONTINUE 3. Doesn’t tell youuse other non insulin agents before use prandial insulin since >80-90 % (conservative) of type 2 pts won’t require bolus insulin if on GLP-1 RA with SGLT-2 inhibitor +/- other
40 30 20 10 0 Obese <140 <240 <120 <100 <280 <320 <360 <400 >400 <200 <160 <180 NGT IGT T2DM INSULIN SECRETION / INSULIN RESISTANCE (DISPOSITION) INDEX DURING OGTT- Lose 80% of function by DX Lean ∆ INS/ ∆ GLU ÷IR 2-Hour PG(mg/dl)
SUMMARY Individuals with IGT: • Are maximally/near-maximally insulin resistant • Have lost ~80% of their beta cell function (DeFronzo) • Have lost significant beta cell mass –but not as much as most believe BUT, note, Lose Mass, but not to same degree as Function