Download
1 / 22
220 likes | 325 Views
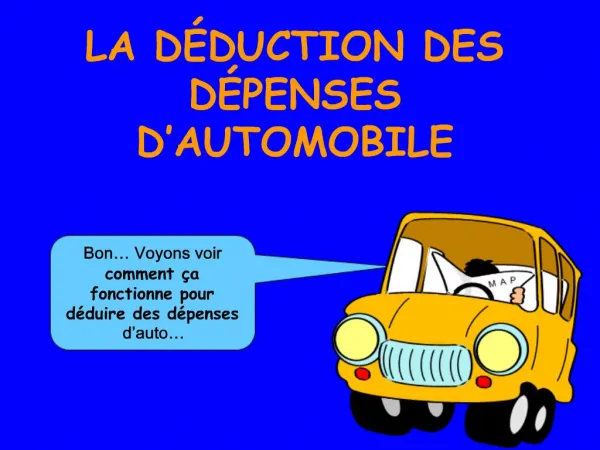
D iabetes RE duction A ssessment with ramipril and rosiglitazone M edication (DREAM) trial. Worldwide prevalence of diabetes expected to increase. World Health Organization, 2000 vs 2030. Diabetes prevalence ~171 million in 2000 ~ 366 million in 2030. 140. 155%. 120. 100. 99%.

E N D
Diabetes REduction Assessment with ramipril and rosiglitazone Medication (DREAM) trial
Worldwide prevalence of diabetes expected to increase World Health Organization, 2000 vs 2030 Diabetes prevalence ~171 million in 2000 ~366 million in 2030 140 155% 120 100 99% 102% Diabetes prevalence (in millions) 80 44% 180% 60 40 160% 20 0 W Pacific Africa Americas E Medit Europe SE Asia 2000 2030 World Health Organization. www.who.org.
DECODE: IGT increases mortality risk Diabetes Epidemiology: Collaborative analysis Of Diagnostic criteria in EuropeN = 25,364 aged ≥30 years Diagnosed diabetes (n = 1275) Undiagnosed diabetes (n = 3071) Impaired glucose tolerance (n = 2766)* Normal glucose tolerance (n = 18,252)* 20 Cumulative mortality hazard (%) 10 0 0 2 4 6 8 10 Follow-up (years) *2-hour oral glucose tolerance test (OGTT) IGT = impaired glucose tolerance DECODE Study Group. Lancet. 1999;354:617-21.
DPP: Benefit of diet + exercise or metformin on diabetes prevention in at-risk patients N = 3234 with IFG and IGT, without diabetes 40 Placebo P* 30 Metformin <0.001 31% Cumulative incidence of diabetes (%) 20 Lifestyle 58% <0.001 10 0 0 1.0 2.0 3.0 4.0 Years *vs placebo IFG = impaired fasting glucose Diabetes Prevention Program (DPP) Research Group. N Engl J Med. 2002;346:393-403.
TZDs: Focus on PPAR activation • Reduces insulin resistance • Preserves pancreatic β-cell function • Improves CV risk profile Improves dyslipidemia (HDL, LDL density, or TG) Renal microalbumin excretion Blood pressure VSMC proliferation/migration in arterial wall PAI-1 levels C-reactive protein levels Adiponectin Free fatty acids Inzucchi SE. JAMA. 2002;287:360-72.
TRIPOD: Treating insulin resistance reduces incidence of type 2 diabetes 12.1% 5.4% TRoglitazone In Prevention Of DiabetesN = 236 Hispanic women with gestational diabetes Annual incidence 60 55% RRR HR 0.45 (0.25–0.83)*P = 0.009 Cumulative incidence of new-onset diabetes (%) 40 Placebo 20 Troglitazone 400 mg 0 0 12 24 36 48 60 Follow-up (months) *Unadjusted Buchanan TA et al. Diabetes. 2002;51:2796-803.
TZDs blunt diabetes progression N = 2343 at high risk of diabetes 15 Placebo Metformin 850 mg bid Cumulative incidence of diabetes (%) 10 Lifestyle Troglitazone400 mg/d* 5 0 0 0.5 1.0 1.5 Follow-up (years) 1568 n = 2343 237 739 DPP Research Group.Diabetes. 2005;54:1150-6. *Withdrawn from study after 1.5 years
Potential antidiabetic mechanisms of ACE inhibition Angiotension I Bradykinin ACE/Kininase II Angiotension II Degradation products ACE Inhibitor Angiotension II Bradykinin Nitric oxide Skeletal muscle blood flow Glucose metabolism Henriksen EJ et al. J Cell Physiol. 2003;196:171-9.
HOPE, EUROPA, PEACE: Reduction in new-onset diabetes (placebo-controlled trials) n = 23,340 free from diabetes* at baseline Overall 14% RRR HR 0.86 (0.78–0.95) P = 0.0023 Ramipril 10 mg Perindopril 8 mg Trandolapril 4 mg (all trials) *Not a prespecified end point Dagenais GR et al. Lancet. 2006;368:581-8.
DREAM: Study design Randomized, double-blind 2 × 2 factorial designN = 5269 with IFG and/or IGT, free from CV disease Ramipril 15 mg/d vs placebo AND Rosiglitazone 8 mg/d vs placebo Primary outcome:Diabetes or death from any cause Secondary outcomes I: CV eventsCombined MI, stroke, CV death, revascularization, HF, angina, ventricular arrhythmia Secondary outcomesII: Renal eventsProgression to micro- or macroalbuminuria, or 30% CrCl Secondary outcomesIII: Glucose status Glucose levels,conversion to normoglycemia Follow-up: 3–5 years DREAM Trial Investigators. Diabetologia. 2004;47:1519-27.
DREAM: 2 × 2 factorial design N = 5269 with IFG and/or IGT Rosiglitazone Placebo Ramipril Ramipril + Rosiglitazone Ramipril + Placebo Placebo Rosiglitazone + Placebo Placebo + Placebo Ramipril: 5 mg × 2 months; 10 mg × 10 months; 15 mg thereafter Rosiglitazone: 4 mg × 2 months; 8 mg thereafter DREAM Trial Investigators. Diabetologia. 2004;47:1519-27.
DREAM: Baseline characteristics Age (years) 54.7 (±10.9) Women (%) 58.5 Hypertension (%) 43.5 Hyperlipidemia (%) 35.5 BP (mm Hg) 136/83 (±18.6/11.3) BMI (kg/m2) 30.5 (±5.1) Waist circumference (inches) Men 34.3 (±10.8) Women 32.6 (±11.9) Glucose FPG (mg/dL) 104 (±12.6) IFG (%) 42.4 2-hour (mg/dL) 157 (±25.2) IGT (%) 85.9 DREAM Trial Investigators. Diabetologia. 2004;47:1519-27.
DREAM: Rosiglitazone effect on primary outcome 0.6 Placebo 60% RRR HR 0.40 (0.35–0.46) P < 0.0001 0.5 0.4 Cumulative hazard rate 0.3 0.2 Rosiglitazone 0.1 0.0 0 1 2 3 4 Follow-up (years) No. at riskPlaceboRosiglitazone 26342635 24702538 21502414 11481310 177217 DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
DREAM: Rosiglitazone decreases new-onset diabetes or death N = 5269 Favorsrosiglitazone Favorsplacebo P <0.0001 <0.0001 0.70 0.25 1 1.75 Hazard ratio *Participants may appear in both categories DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
DREAM: Effect of rosiglitazone on primary outcome in key subgroups P* Placebo (% per year) Favors rosiglitazone Favors placebo Gender Male Female Age (years) <50 60+ 50–59 Location North America South America Europe India Australia Glycemic abnormality IFG only IGT only IFG + IGT 9.9 7.6 8.4 9.5 7.7 8.8 8.0 8.6 8.7 7.2 7.0 6.1 14.0 0.6 0.09 0.09 0.14 0.2 0.4 0.6 0.8 1.0 1.2 Hazard ratio (95% CI) *for heterogeneity DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
DREAM: Conversion to normoglycemia with rosiglitazone N = 5269 71% increaseHR 1.71 (1.571.87)P < 0.0001 *FPG < 110 mg/dL and 2-h glucose < 140 mg/dL DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
Rosiglitazone effect on weight and BMI Weight BMI 200 32 196 31 191 lbs kg/m2 187 30 P < 0.0001 P < 0.0001 182 0 0 0 1 2 3 4 5 0 1 2 3 4 5 Follow-up (years) Rosiglitazone Placebo DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
Rosiglitazone effect on waist and hip measurements WHR Circumference 45.3 0.94 Hip 43.7 0.92 42.1 P < 0.0001 inches 40.6 Waist 0.90 P < 0.0001 39.0 P = NS 37.4 0.88 0 0 0 1 2 3 4 5 0 1 2 3 4 5 Follow-up (years) Rosiglitazone Placebo WHR = waist-hip ratio DREAM Trial Investigators. Lancet. 2006;368:1096-1105.
DREAM: Ramipril effect on primary outcome 0.6 9% RRRHR 0.91 (0.81–1.03) P = 0.15 0.5 Placebo 0.4 Cumulative hazard rate 0.3 0.2 Ramipril 0.1 0.0 0 1 2 3 4 Follow-up (years) 26462623 25102498 22772287 12401218 200194 No. at riskPlaceboRamipril DREAM Trial Investigators. N Engl J Med. 2006;355:1551-62.
DREAM: Ramipril effects on glycemic categories P = 0.006 DREAM Trial Investigators. N Engl J Med. 2006;355:1551-62.
DREAM: Safety Rosiglitazone vs placebo • Increased incidence of HF* (0.5% vs 0.1%, P = 0.01) • No cases of fatal HF • No difference for other CV events • Increased incidence of peripheral edema(6.8% vs 4.9%, P = 0.003) • 4.9-lb weight gain (P < 0.0001) • Increased hip circumference (0.71 in, P < 0.0001) • No difference in waist circumference • Decreased waist-hip ratio (P < 0.0001) • No adverse hepatic effects • Alanine aminotransferase (ALT) levels 4.2 U/L at 1 year (P < 0.0001) Ramipril vs placebo • No adverse hepatic effects • ALT levels 1.1 U/L at 1 year (P = 0.004) DREAM Trial Investigators. Lancet. 2006;368:1096-1105; N Engl J Med. 2006;355:1551-62. *Adjudicated
DREAM results: Summary Rosiglitazone • 60% RRR in new-onset diabetes or death (P < 0.001); NNT = 7 • Benefit consistent across ethnicity, gender, and age • Increased conversion to normoglycemia* vs placebo (50.5% vs 30.3%) (HR 1.71, P < 0.0001) • BP vs placebo (1.7/1.4 mm Hg; P < 0.0001) Ramipril • 9% RRR in new-onset diabetes or death (P = 0.15) • Increased conversion to normoglycemia* vs placebo (42.5% vs 38.2%) (HR 1.16, P = 0.001) • BP vs placebo (4.3/2.4 mm Hg; P < 0.001) • When ACEIs are indicated, improved glucose metabolism may be added benefit DREAM Trial Investigators. Lancet. 2006;368:1096-1105;N Engl J Med. 2006;355:1551-62. *FPG < 110 mg/dL and 2-h glucose < 140 mg/dL