Download
1 / 15
870 likes | 7.46k Views
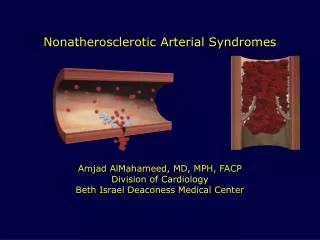
Thromboangiitis Obliterans Buerger’s Disease. Nonatherosclerotic segmental inflammatory disease affecting small and medium-sized arteries/veins in upper/lower extremities Categorized as a vasculitis Highly inflammatory thrombus with sparing of vessel wall

E N D
Thromboangiitis ObliteransBuerger’s Disease • Nonatherosclerotic segmental inflammatory disease affecting small and medium-sized arteries/veins in upper/lower extremities • Categorized as a vasculitis • Highly inflammatory thrombus with sparing of vessel wall • Most commonly seen in young men with heavy tobacco use
History • 1879 (von Winiwarter): first case of 57yo male with foot pain leading to gangrene • Pathologic specimen showed intimal proliferation, thrombosis, and fibrosis • Suggested that vessel changes distinct from atherosclerosis • 1908 (Buerger): detailed description of 11 amputated limbs at Mt. Sinai with endarteritis and endophlebitis • 1928 (Allen & Brown): 200 cases at Mayo Clinic • Jewish men that were heavy smokers
Epidemiology • More prevalent in Middle and Far East than in N. America • Mayo Clinic showed decline from 104/100k in ’47 to 12/100k in ’86 • International series widely variable in terms of causes of limb ischemia • Western Europe 0.5-5.6% • Poland 3% • E.Germany 6.7% • Czech Republic 11.5% • Yugoslavia 39% • India 45-63% • Women have increasing incidence • Published series prior to 1970: 1-2% • 23% at Cleveland Clinic (1970-1987) • 19% at OHSU (1987)
Etiology • UNKNOWN! • Distinct from other vasculitis • 1. thrombus is highly cellular with less intense cellular reaction in vessel wall • 2. normal immunologic markers • Strong association with smoking • No gene association found yet • Conflicting studies regarding hypercoagulable states • Increased urokinase plasminogen activator • Impaired endothelium-dependent vasorelaxation • Immunologic mechanisms may be contributory • Increased cellular sensitivity to Types I and III collagen
Pathology • Inflammatory thrombosis that affects arteries and veins • Acute-phase • Inflammation involving all layers of vessel wall with occlusive thrombosis • Microabscesses & multinucleated giant cells • Intermediate phase • Progressive organization of occlusive thrombus • Prominent inflammatory infiltrate within thrombus • Chronic phase • Extensive recanalization • Adventitial & perivascular fibrosis • Segmental in distribution • Skip areas noted • Rare to involve cerebral, coronary, renal, or mesenteric vessels • Non-necrotizing involvement of vessel wall
Clinical Features • Classic presentation • Young male smoker with onset of symptoms before age 40-45 • Ischemia of distal small arteries and veins • Cleveland Clinic 1990: presenting signs/symptoms in 112 patients • Initial site of claudication is arch of foot • Usually >2 limbs involved • Not uncommon to see angiographic findings in asymptomatic limbs • Upper extremity involvement distinguished from atherosclerosis
Clinical Features • Classification Systems • Major Criteria • Onset of distal extremity ischemic symptoms prior to aqe 45 • Tobacco abuse • Undiseased arteries proximal to brachial & popliteal • Objective documentation of distal occlusive disease by plethysmography • Exclusion of proximal embolic source, trauma, autoimmune disease, hypercoagulable state, atherosclerosis • Minor Criteria • Migratory superficial phlebitis • Raynaud’s syndrome • Upper extremity involvement • Instep claudication • No typical lab abnormalities
Arteriography • Involvement of small and medium-sized vessels • Digital arteries of fingers and toes • Palmar, plantar, tibial, peroneal, radial, and ulnar • Segmental occlusive lesions • More severe disease distally • Corkscrew collaterals • Normal proximal arteries
Treatment • STOP ALL SMOKING! • Complete abstinence is the only way to stop progression of disease and prevent future amputation • All other therapies are palliative • Prostaglandin (iloprost) • Calcium channel blockers for vasospasm • Pentoxifylline • Sympathectomy • Thrombolytic therapy • Surgical revascularization • Limited due to skip lesions and distal disease • Usually <10% patients in series are bypass candidates • 5 year patency 49% in large series from Europe • 67% in those that stopped smoking and 35% in smokers
Nonatheroslerotic, segmental, inflammatory disease affecting small and medium sized arteries and veins of upper and lower extremities • Typically occurs in younger males with heavy tobacco use • Smoking cessation is key to therapy