Download
1 / 17
170 likes | 545 Views
RETT SYNDROME AN UPDATE. Rosemary Marks Developmental Paediatrician Starship Childrens Hospital. SUMMARY. Background Recognition of Rett syndrome Management of Rett Syndrome. RETT SYNDROME. Described in 1966 by Andreas Rett First described in English by Hagberg in 1983

E N D
RETT SYNDROMEAN UPDATE Rosemary Marks Developmental Paediatrician Starship Childrens Hospital
SUMMARY • Background • Recognition of Rett syndrome • Management of Rett Syndrome
RETT SYNDROME • Described in 1966 by Andreas Rett • First described in English by Hagberg in 1983 • 1999 – mutations in MECP2 gene reported • Methyl CpG binding protein 2 • CDKL5 cyclin-dependent kinase like 5 • Netrin G1 • 1 in 10000 females
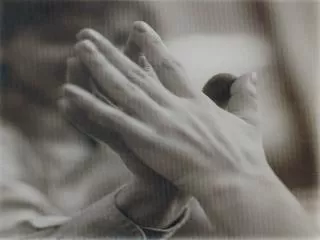
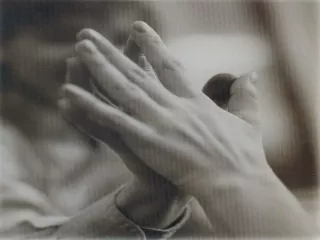
RETT PHENOTYPE • Rett syndrome • Normal early development* • Withdrawn autistic behaviour; loss of language • Loss of hand-skills; stereotypic hand movements • Deceleration of head growth • Seizure disorder • Progressive course with well described stages • Caution re prognosis as broader phenotype recognised
RECOGNITION • Think Rett • Listen to the parents • All girls with autistic behaviour • All girls with history of developmental stagnation or loss of skills around one year of age • Boys with neonatal encephalopathy
Clinical criteria for classical Rett Necessary criteria 1. Normal prenatal and perinatal history* 2. Normal psychomotor development for the first 6 months 3. Normal head circumference at birth 4. Postnatal deceleration of head growth in most individuals 5. Loss of purposeful hand skills between 6 months and 2½ years 6. Hand stereotypies 7. Evolving social withdrawal, communication dysfunction, loss of acquired speech, and cognitive impairment 8. Impairment or deterioration of locomotion
Clinical criteria for classical Rett Supportive criteria 1. Breathing disturbances during waking hours 2. Bruxism 3. Impairment of sleeping pattern from early infancy 4. Abnormal muscle tone associated with muscle wasting and dystonia 5. Peripheral vasomotor disturbances 6. Progressive kyphosis or scoliosis 7. Growth retardation 8. Hypotrophic small and cold feet and/or hands
Clinical criteria for classical Rett Exclusion criteria 1. Evidence of a storage disorder including organomegaly 2. Cataract, retinopathy, or optic atrophy 3. History of perinatal or postnatal brain damage 4. Confirmed inborn error of metabolism or neurodegenerative disorder 5. Acquired neurological disorder due to severe head trauma or infection
Early normal development • Is it really? • Abnormal quality of movement • Tongue protrusion • Postural stiffness • Asymmetric eye open/close • Abnormal hand and finger movements • Abnormal facial expression/smile • Tremor • Stereotyped body movements Einspieler et al. Pediatr Res 57: 696–700, 2005 Burford, B. Brain & Development 27 (2005) S3–S7
What else could it be? • Angelman syndrome • Prader-Willi syndrome • Autism
RETT SYNDROMEMANAGEMENT • Intervention programmes • Nutrition • Long QT • Sleep problems • Epilepsy • Breathing dysfunction • Scoliosis
SLEEP PROBLEMS • Consider relationship to epilepsy and breathing dysfunction • Sleep hygiene • Melatonin • Pipamperone (5-hydroxytryptophan antagonist) – case report
EPILEPSY • Valproate • No RCTs specific to Rett syndrome
BREATHING DYSFUNCTION • Range of abnormal breathing behaviours • Forceful/Valsalva • Feeble • Apneustic • Potential treatments • Magnesium • Carbogen (a mixture of 5% carbon dioxide and 95% oxygen) • RCTs needed
SCOLIOSIS • Physiotherapy and positioning • No evidence that bracing is effective • Surgery • Guidelines for Management of Scoliosis in Rett Syndrome Patients Based on Expert Consensus and Clinical Evidence • Parental experiences of scoliosis management in Rett syndrome Downs et al. Spine, 34(17) E607-E617, 2009 doi: 10.1097/BRS.0b013e3181a95ca4 Ager et al. Disability & Rehabilitation, 31(23) 1917-1924, 2009