Download
1 / 31
310 likes | 390 Views
Malaria Myths and Misadventures: Keeping Travellers Safe from a Deadly Disease. Karen L McClean MD FRCPC Division of Infectious Diseases. Every 30 seconds, a child dies of malaria…. Malaria in Canadian Travellers. In the 1990s …

E N D
Malaria Myths and Misadventures: Keeping Travellers Safe from a Deadly Disease Karen L McClean MD FRCPC Division of Infectious Diseases
Malaria in Canadian Travellers • In the 1990s … • 9 Canadian travellers died from malaria (+/- unreported / undiagnosed cases) • We continue to see (on average)… • 538 cases of malaria each year • one death from malaria each year • In 2006 in Saskatchewan… • 2 patients admitted to ICU for severe / complicated malaria
Fact or Myth? • Death can occur in as little as 24-48 hours from onset of the first symptoms. Fact! • Progression from mild to severe disease can be very rapid and unpredictable.
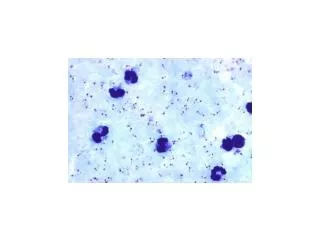
19 year old woman • Travel to Ghana • Doxycycline for malaria prophylaxis • Discontinued because of vivid dreams • First symptoms: April 18 (after return home) • 1st visit: April 18…’viral’, no testing • 2nd visit: April 19…insisted on testing • Smear examined April 20 am…’rare parasites’ • Repeat blood smears drawn April 20 am…20% parasitemia! • IV quinine not available (at designated regional site)….could not be located • Transferred.…first dose of quinine at 2400 hours
Delay…. • 62 hour treatment delay • Failure to consider dx - 24 hours • Failure to obtain test results - 24 hours • Failureto access drug - 14 hours
37 year old woman • Travel to Tanzania for 10 day safari • Chose not to use anti-malarials • Concerned about side effects • First symptoms: July 4 (Tuesday) • 1st visit: July 4 pm….’viral’, no testing • 2nd visit: July 6…. smears sent to referral lab by bus • 3rd visit: July 7…. Worse, dyspneic, no results available from blood smear • July 7, 2000 hours…Severely ill, transfer arranged, first dose of IV quinine at 0200
Delay… • 88 hour delay in treatment! • Failure to consider dx – 48 hours • Failure to obtain test results – 40 hours
Malaria • Possible malaria should be considered a medical emergency even if symptoms are mild. • Prompt diagnosis is medically (and medico-legally) essential. • Blood smear results should be available in 4-6 hours – if not, transfer of the patient to a site that can provide results promptly is necessary.
Fact or Myth? • People who grew up with malaria do not require chemoprophylaxis because they are immune. Myth!
Immunity to Malaria • Develops slowly and only after multiple episodes of clinical disease. • Is incomplete and never fully protective against disease, severe disease or death. • Is transient – and lost within 3-6 months of leaving an area of continuous exposure.
VFRs: high risk group • VFRs = “visiting friends and relatives” • Travel home to endemic areas • Often don’t seek pre-travel advice • Do not perceive themselves at risk • Consider malaria a minor disease • Consider themselves immune • Periodic health exam can provide a good opportunity to ask about possible future travel.
Fact or Myth? • Mefloquine has a high rate serious side effects. Myth!
Chemoprophylaxis • Chloroquine – “tried and true”…but… • Widespread resistance: useful only in some areas of Caribbean, Central America, Middle East • Mefloquine – lots of “bad press” • Malarone - “new kid on the block” • Expensive, increasing reports of resistance • Doxycycline – “best kept secret” • Photosensitivity: little problem at 100 mg/d • Yeast infections: standby treatment
Mefloquine • 1984-1995 • 16 million people treated • 1,574 reported adverse events • 18 cohort studies • Serious adverse events • mefloquine: 1/13,300 • chloroquine: 1/13,600 • Neuropsychiatric AE’s • Peace corp volunteers: 1:910,000 • Swiss travellers: 1: 81,000 • UK travellers: 1: 96,000
Mefloquine A/Es Retrospective studies • 2.6X more non-responders in Mefloquine group • 42% of mefloquine SAE’s occurred in patients with clear contraindications to mefloquine
Mefloquine • There are many anecdotal reports of the “mefloquine ruined my life” variety … but • There is no evidence for long term health consequences of mefloquine.
Mefloquine • Mefloquine does have adverse effects…as do all anti-malarials. • Contraindications must be respected. • Psychiatric illness including depression • Arrhythmias, drugs prolonging QT interval • Seizure disorder
Mefloquine • Can be safely used if contraindications are respected. • Loading dose regimen can be used to help identify travellers who may not tolerate MFQ – and provide an opportunity to chose alternate chemophrophylaxis. • 250 mg daily x 3 days then weekly • Rapidly achieves steady state (vs. 7 weeks with weekly dosing)
Fact or Myth • For travellers concerned about the cost of antimalarials, these drugs are readily available at low cost overseas. Fact …but….
Counterfeit Drugs • Fake drugs make up 10%-15% of the global market. • In parts of Africa and Asia: >50% • China: 2001 • 192,000 patients deaths attributed to fake drugs • 1,300 factories closed www.cdc.gov/malaria/travel/counterfeit_drugs.htm
Counterfeit Drugs • Counterfeit drugs can be / include: • Inactive compounds • Active but subtherapeutic compound • Other (non label) drugs including sulpha compounds • Harmful / toxic compounds • Counterfeit drug makers include just enough active ingredient to ‘trick’ field tests • Counterfeiters can produce convincing ‘quality assurance’ holograms and product labels.
Protecting travellers… • Awareness…. • Counterfeit drugs are common • Counterfeit drugs can’t be visually differentiated from true drugs • The problems is worldwide… but particularly prevalent in developing countries • Antibiotics and antimalarials are prime targets for counterfeiters
Fact or Myth • DEET should be used in concentrations of < 30% (10% for children) because of risks of toxicity. That depends!
DEET Toxicity • <30% limit recommended by PMRA (10% for children) • Based on mathematical modelling • No consideration of risks of arthropod borne diseases • Toxicity reports in children • Seizures – due to oral ingestion of DEET not topical application
DEET • Efficacy & duration of action increase with concentration • For protection against arthropod borne diseases, recommend: • 35% concentration • Extended-release formulations • i.e. Ultrathon by 3M • Labelled for 8 hour duration – but reapply sooner if biting observed • Available on-line from US distributors • Can be imported into Canada for personal use • Children: single application of 35% DEET results in less overall exposure than repeated application of 10% DEET • When used as directed…DEET has an excellent safety record
DEET • Preferred agents (best efficacy) • DEET • Picardin (Bayrepel, Autan) • available in Europe • Equivalent efficacy to DEET • Modestly effective • Soybean oil (Bite Blocker) • Lemon Eucalyptus oil (Off Botanicals) • Not effective • Citronella and other ‘natural’ repellents are NOT effective.
Fact or Myth? • I didn’t hear or see mosquitoes so I wasn’t at risk. Myth!
Anopheles mosquitoes • Anopheles mosquitoes are inconspicuous • Active from dusk to dawn • Rest during the day • Noiseless fliers CDC photo
Malaria prophylaxis • Chemoprophylaxis (90-95% effective) plus • Personal protective measures • Insecticide treated bed nets • DEET • Why prophylaxis? • To prevent DEATH
Common themes in malaria deaths… • Failure to use prophylaxis • VFRs (visiting friends and relatives) • Concern about side effects, cost, inconvenience • Use of inappropriate prophylaxis • Wrong drug for destination • Inappropriate sources for advice • Counterfeit drugs • Diagnostic delays • Failure to seek medical advice promptly • Failure to consider the diagnosis • Failure to order appropriate tests • Failure to handle malaria diagnostic tests in a timely manner