Download
1 / 63
650 likes | 852 Views
ARACHIDONIC ACID, PROSTANOID METABOLISM and DRUGS AFFECTING INFLAMMATORY DISEASE. Introduction Biosynthesis Inhibition of Biosynthesis Physiology of the Prostanoids NSAIDs Adverse Effects - Correlation with Physiology Corticosteroids as Antiinflammatories Other Anti-inflammatories/DMARDs.

E N D
ARACHIDONIC ACID, PROSTANOID METABOLISMand DRUGS AFFECTING INFLAMMATORY DISEASE • Introduction • Biosynthesis • Inhibition of Biosynthesis • Physiology of the Prostanoids • NSAIDs • Adverse Effects - Correlation with Physiology • Corticosteroids as Antiinflammatories • Other Anti-inflammatories/DMARDs M.E. Maguire Pharmacology W218 mem6@
TAKE HOME MESSAGES • The pharmacological actions of drugs affecting prostanoids are predictable if you understand the basic physiology of prostanoid action • The adverse effects of drugs affecting prostanoids are predictable if you understand the basic physiology of prostanoid action
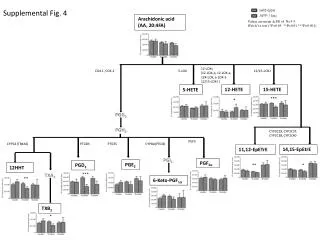
Prostanoid Metabolism Membrane X Glucocorticoids Cyclooxygenase PGH Synthase Chemotactic Lipids Arachidonic Acid 5-Lipoxygenase 12-Lipoxygenase 15-Lipoxygenase ??? X NSAIDs 12-H(P)ETE 15-H(P)ETE Lipoxins PGX 5-H(P)ETE Leukotrienes PGG/PGH Endoperoxides PGE2 PGF2a PGI2 Prostacyclin TxA2 Thromboxane
Prostanoids • Made from arachidonic acid by cyclooxygenase • Autacoids • Not stored • Made & released on demand • Act locally, do not circulate
Inhibition of Prostanoid Metabolism • NSAID • Non-Steroidal Anti-Inflammatory Drug • Inhibit cyclooxygenase • Prevent biosynthesis of ALL prostanoids • Cyclooxygenase • Two isoforms - COX-1/COX-2 • May be a COX-3 • Some NSAIDs can differentially inhibit isoforms • Who cares?
COX-1 • Constitutive • Tissues • Blood cells - platelet aggregation • Kidney - BP and distribution • Stomach - acid & mucous secretion • Smooth muscle - contraction (usually) • Hypothalamus - temperature set point (fever) • Downstream prostaglandin synthases • Also constitutive • Generally soluble cytosolic enzymes • Currently unknown implications for transport & release of prostanoids
COX-2 • Expression is regulated • Induced by • Cytokines • Endotoxins • Mitogens • Repressed by • Glucocorticoids (cortisol/prednisone) • Clearly involved in inflammatory processes • Tissues • Epithelial cells (gut) • Migratory blood cells, especially macrophages • Prostaglandin Synthases • Inducible • Generally membrane-bound proteins • Again, unknown implications for transport & release
Prostanoid Physiology 1 • Platelets and vascular endothelium - COX-1 • Plateletstimulation releases AA • Platelets make Thromboxane A (TxA) via COX-1 • TxA aggregates platelets & vasoconstricts • Most vascular endotheliumhas NO phospholipase and thus releases no AA • Vascular endothelium sees AA from platelets, makes PGI (prostacyclin) but largely via COX-2 • PGI disaggregates platelets & vasodilates • Balance helps determine • Initiation of clot formation • Formation of plaques
Prostanoid Physiology 1 • Platelets (COX-1) and vascular endothelium (COX-1 & COX-2) • Lung microvessels and coronary arteries uniquely have high level of phospholipase to make AA, producing PGI • Regulated by pO2 • PGI dissolves microclots in lung vessels (good!) • PGI dilates coronary arteries (good!) • Atherosclerosis • PGI metabolites in blood 20X • Aspirin inhibits BOTH COX-1 and COX-2 • Irreversibly acetylates enzyme • Other NSAIDs are reversible
Prostanoid Physiology 1 • Platelets and vascular endothelium - COX-1 • Aspirin & platelets • Platelets cannot synthesize protein • Half-life of 10-11 days • Once inhibited, new cells must be made to get COX-1 and thus TxA back for aggregation • Aspirin & vascular endothelium • Endothelium turns over rapidly • New COX-1/COX-2 made rapidly • Pharmacokinetics • Platelets see the highest [Aspirin] in portal vein • Aspirin diluted with circulation in blood • Rapid metabolism of aspirin (T1/2 = 10-15 min) • So endothelium sees much lower [Aspirin], therefore less effect
Renal Vasoconstriction Circulation Increased renal synthesis of PGE/PGI Renal Vasodilatation & Distribution Renin release Prostanoid Physiology 2 • Kidney blood flow - COX-1 versus COX-2???? Angiotensin II Norepinephrine
Rheobatrachus vitellinus extinct 1989 Prostanoid Physiology 3 • GI Tract - COX-1 • PGE/PGI inhibit acid secretion from all known stimuli • PGE/PGI stimulate mucous and bicarbonate secretion • Unimpeded acid secretion and decreased mucous & bicarbonate production can “cause” ulcers • Administration of NSAIDs removes regulatory feedback on gastric acid secretion
Prostanoid Physiology 4 • Macrophages, neutrophils, etc.- COX-2 • Prostanoids mediate aspects of inflammation and pain • Chemoattractants, recruit more inflammatory cells • COX-2 upregulated by inflammatory processes
Prostanoid Physiology 5 • Where else is COX-2 involved? • Gut immune surveillance - essential • Cardiovascular system, not completely understood • Indirect through effects of PGI/TxA • Some vasculature has COX-2 mediated PGI production • Cancer prevention and treatment • Colorectal cancer – good preliminary evidence that COX-2 inhibitors are effective in primary treatment and reduce spread • Numerous large scale clinical trials WERE evaluating COX-2 selective inhibitors as adjunct treatment for cancers of the colon, lung, breast, esophagus, pancreas, liver, and cervix
NSAIDs • Multiple classes • COX-1 selective • Aspirin - only irreversible NSAID • Ibuprofen (Advil) • Indomethacin (Indocin) • Most others • COX-1 = COX-2 • Naproxen (Aleve) • COX-2 selective (somewhat selective, plus longer half-lives) • Celecoxib (Celebrex) • Rofecoxib (Vioxx) • etc.
NSAID Adverse Effects • PREDICTABLE from Physiology • Ulcers - GI effects on acid/mucous secretion • Renal nephropathy - Unimpeded vasoconstriction • Bleeding - platelets
NSAID Adverse Effects • COX-1 versus COX-2 selective inhibitors • COX-2 have 5-10X incidence of ulceration • COX-2 have similar incidence of renal nephropathy • COX-2 contributes some PGI/prostacyclin from vascular endothelium • Therefore chronic treatment tips balance slightly towards platelet aggregation • COX-2 use associated with a 3X+ in MI/stroke • COX-2 costs 10-30X more • Little current use for COX-2 inhibitors • Celecoxib only COX-2 left on market
Vioxx Recall Data • NSAID use Cases Adjusted OR (95% CI) • Remote use 4699 1.00 • Recent use 1728 1.14 (1.06-1.22) • Current CHRONIC use • Celecoxib 126 0.86 (0.69-1.07) • Ibuprofen 674 1.09 (0.99-1.21) • Naproxen 369 1.18 (1.04-1.35) • Rofecoxib ≤ 25 mg 58 1.29 (0.93-1.79) • Rofecoxib > 25 mg 10 3.15 (1.14-8.75) • Other NSAIDs 535 1.16 (1.04-1.30)
Other NSAID Effects • May decrease incidence of gastric cancers • Probably related to prostanoid effects on gastrin • Increased NSAID use associated with decrease in Alzheimer’s incidence • Apparently decreases amyloid plaque deposition • May not be due to decreased inflammatory insult • NOT related to COX inhibition, only a subset of NSAIDs work • Decreases production of Ab42 in brain by altering specificity of g-secretase
FDA Warning Letters • Patients in a colon cancer clinical trial taking 400 mg of Celebrex twice daily had a 3.4 times greater risk of CV events compared to placebo • For patients in the trial taking 200 mg of Celebrex twice daily, the risk was 2.5 times greater • The average duration of treatment in the trial was 33 months • A similar ongoing study comparing Celebrex 400 mg once a day versus placebo, in patients followed for a similar period of time, has not shown increased risk
NSAID Use • These are generally safe drugs • They pose no significant risk of increased cardiovascular events when used sporadically for headache, aches and pains or short-term pain relief in otherwise healthy individuals • They ALL (including COX-1 selective like ibuprofen and non-selectives like naproxen) will increase the risk of stroke/clots when used chronically • The longer the use, the higher the risk • It’s about 1.0-1.4X for ibuprofen/naproxen • and 3-4X for COX-2 selectives
NSAID Use • They do NOT, despite the court decision against Merck and Vioxx, increase the risk of arrhythmias • In patients who are at risk for stroke, these medicines should not be used chronically, and should be used cautiously for short term use • Acetaminophen is by far the better choice • In patients with severe arthritic pain, these are still the medicines of choice. For those with severe arthritis and who have concomitant GI problems with NSAIDs, cautious use of COX-2 selectives may be warranted
NSAID Use • Anyone getting NSAIDs chronically (even for 2 weeks) should also get a proton-pump inhibitor • Keep taking that quarter aspirin tablet • Essentially, this whole problem was caused by drug companies promoting use of COX-2’s for everyone instead of just those with GI problems, and by physicians who used them that way
A Word about ACETAMINOPHEN • NSAIDs have three basic effects • Antiinflammatory • Antipyretic (decrease fever) • Analgesic • ACETAMINOPHEN is NOT an NSAID • Mechanism of action unknown • NOT by inhibition of COX • NOT ANTI-INFLAMMATORY • Analgesic & Antipyretic ONLY • FREE QUESTION • Which of the following is NOT antiinflammatory?????
Glucocorticoids Hypothalamus • Essential for life • Circulating hormone • From adrenal cortex, made on demand from cholesterol • Controlled by classic negative feedback loop CRH X Anterior Pituitary Circulation ACTH Adrenal Cortex ACTH - Adrenocorticotrophic hormone CORTISOL Adrenal cortex trophic hormone
Cortisol 1 • Glucocorticoids • Glucocorticoids are NOT sex steroids like estrogen or testosterone • Fundamental to energy metabolism • MANY other roles • Cytosolic receptor • Nuclear transcription factor • Regulates MANY genes
Cortisol 2 • Energy Metabolism • Insulin, glucagon and cortisol are the three primary hormones controlling energy metabolism • In periphery,cortisol • Breaks down protein and lipid • Causes underutilization of glucose • In liver, cortisol • Enhances amino and fatty acid conversion to glucose and glycogen • Can cause hyperglycemia from production of too much glucose as well as a negative nitrogen balance from amino acid catabolism
Cortisol 3 • Antiinflammatory • Reduces vascular permeability and edema • Decreases prostanoid production by preventing release of AA • Suppresses lymphoid tissue • Causes lymphocyte apoptosis - leukopenia • Basis for use in cancer chemotherapy • Suppresses immune response • Stress response • Stress increases cortisol levels proportionally to stress • Without cortisol, cannot respond to stress
Cortisol 4 • ADVERSE EFFECTS • Acute one-time administration of virtually any dose of cortisol is without significant incidence of any adverse effect • SHORT-TERM administration of even extremely high doses of cortisol has little or no significant long-term consequence • “Short-term” is defined as 7-10 days without dose tapering or up to a month with dose tapering • HOWEVER, chronic use has potentially severe adverse effects
Cortisol 5 • ADVERSE EFFECTS - ON CHRONIC USE • Diabetes insipidus • Muscle wasting/atrophy • Obesity • Breaks down “white” fat, stimulates and redistributes “brown” fat • Osteoporosis • Stimulates Ca2+ loss & bone breakdown • May be irreversible • Growth suppression • Inhibits growth hormone secretion • May be irreversible • Vascular necrosis - mechanism ??
Cortisol 6 • ADVERSE EFFECTS - ON CHRONIC USE • Cataracts • Occur more often in young • Usually not reversible • Suppresses response to infection • via effects on lymphoid cells • Suppresses menstruation • Psychic effects • Short-term high dose is euphoric • Often used in hospice care with terminal patients • Long-term induces often irreversible psychosis • Thinning of skin • Significant thinning, usually irreversible • Atrophy of Adrenal Cortex
Cortisol 7 • USE • Ubiquitous • Helps an incredible number of conditions • Safe for short-term use • Potentially problematic in long-term use • But can be critical for treatment • Often no alternative
Summary of NSAIDs & Glucocorticoids • PROSTANOIDS are Autacoids • COX-1 & COX-2 • Cell types • Selective inhibition • NSAIDs • Inhibit ALL prostanoid synthesis • Generally safe • Adverse effects can be severe • Adverse effects predictable from physiology • Cortisol - Glucocorticoids • Energy metabolism - essential • Useful for many conditions • Safe short-term, potential toxicities long-term • Acetaminophen NOT anti-inflammatory, NOT an NSAID
DMARDs & Immunosuppressants • Disease Modifying Anti-Rheumatic Drugs (DMARDs) • Appear to slow or halt progression of inflammatory disease • Mechanisms of action unclear in some cases • Immunosuppressants • Prevent progression? • Overlap with DMARDs • Reverse disease progression?
DMARDs • Hydroxychloroquine (Plaquenil) • Gold salts • Sulfasalazine • Used primarily in Europe • ALL take weeks/months to show effect
Hydroxychloroquine (Plaquenil) • Anti-malarial • Mechanism unknown • Preferred over chloroquine because of decreased ocular toxicity • No really good clinical trials
Hydroxychloroquine (Plaquenil) • Well tolerated for malaria, but higher doses in RA can be toxic • Ototoxicity • Retinopathy • Accumulates in melanin rich tissues • Avoid combining with gold and most NSAIDs • Severe dermatitis • Glucose-6-phosphatase deficiency • Hemolysis • 10% of African-American males • Liver metabolism easily saturated
Gold Salts • Gold conjugated to various organic salts • IM or Oral • IM preferred, get 4X the synovial Au concentration • Mechanism unknown • Has given way to methotrexate and immunosuppressants, but may be useful when other therapies fail
Gold Salts • 15% dermatological reactions • 50% transient proteinuria • 5-10% Decreased kidney function • 1-3% show proximal tubular damage, usually reversible • 1% thrombocytopenia (withdraw immediately) • Other blood dyscrasias • TERATOGENIC
Sulfasalazine (Azulfidine) • Antibiotic • Metabolized in gut to: • Sulfapyridine • Sulfonamide antibiotic • GI toxicity • 5-Amino-Salicylate • Essentially aspirin/NSAID • Toxicities • Nausea, fever, rash, arthralgias (20%) • Glucose-6-phosphatase deficiency • Not particularly effective
IMMUNOSUPPRESSANTS • Methotrexate (Rheumatrex) • Leflunomide (Arava) • Etanercept (Enbrel) and Infliximab (Remicade) • Anakinra (Kineret) • Azathioprine (Imuran) • Cyclophosphamide (Cytoxan)
Methotrexate • Folic acid antagonist • Inhibits 1-carbon transfers • Thymidine biosynthesis
Methotrexate • Effective dose in RA much less than for chemotherapy • Suggests mechanism of action might not be on DNA synthesis • May show effects in 4-6 weeks, sooner than other DMARDs/Immunosuppressants • While minimal clinical trial data exist, now accepted as a mainline drug for RA
Methotrexate • Toxicities • Weight loss, GI disturbances • Less frequent with doses for RA • Interstitial pneumonitis (2%) • Baseline and routine chest x-rays required • Lower incidence in arthritis because of lower dose • HIGHLY TERATOGENIC • Men also
Leflunomide • Inhibits dihydroorotate dehydrogenase • Prevents pyrimidine and specifically UMP biosynthesis • May also affect some tyrosine kinases????
Leflunomide • Causes preferential cell arrest of autoimmune lymphocytes • Stimulated lymphocytes must increase ribonucleotide levels from 8 to 16-fold before proceeding from the G1 to the S phase of the cell cycle • Low levels of ribonucleotides cause cell cycle arrest
Leflunomide • T1/2 is 15 days • Given as large loading dose • Followed by smaller maintenance doses
Leflunomide • Toxicities • No major limiting side effects at present • Alopecia • Headache • Transient mild diarrhea • Abnormal liver transaminase activity • TERATOGENIC • No actual data, but considered to be teratogenic because of mechanism of action
Etanercept, Infliximab and Adalimumab • All antagonize TNF • Etanercept (Enbrel) • Ligand binding domain of human TNF receptor + Fc portion of human IgG1 • Infliximab (Remicade) • Mouse monoclonal antibody targeted to TNF + Human IgG1 sequence • Adalimumab (Humira) • Human monoclonal antibody (recombinant IgG1) targeted to TNF
Etanercept, Infliximab and Adalimumab • Proteins • Limited to blood volume • Antibody development???? • Concomitant treatment with methotrexate likely decreases immune response to chimeric proteins • Bind TNF with very high affinity • [TNF] in blood goes to zero • Concentration gradient sucks tissue TNF into blood • Complex eventually eliminated by kidney and/or metabolism • Concept same as anti-digoxin antibodies