Download
1 / 39
400 likes | 427 Views
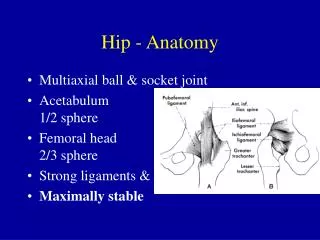
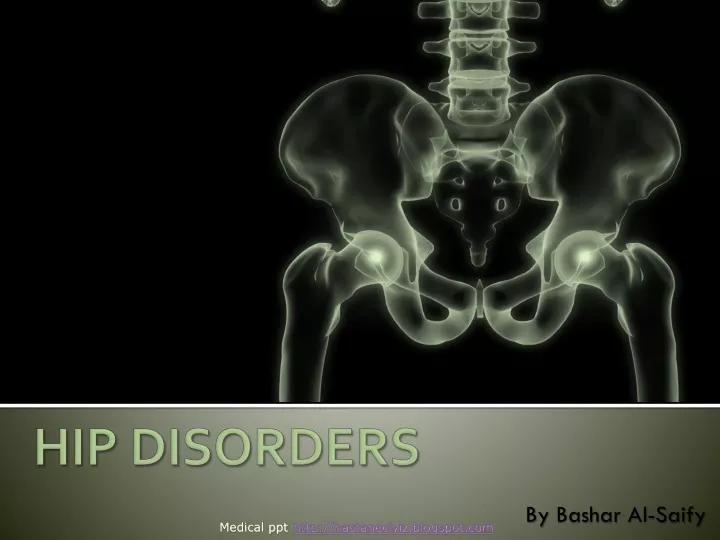
By Bashar Al- Saify. HIP DISORDERS. Medical ppt. http://hastaneciyiz.blogspot.com. Hip Disorders :. Slipped capital femoral epiphysis (SCFE) Traumatic hip dislocation Osteoarthritis. Slipped capital femoral epiphysis (SCFE).

E N D
By Bashar Al-Saify HIP DISORDERS Medical ppt http://hastaneciyiz.blogspot.com
Hip Disorders : • Slipped capital femoral epiphysis (SCFE) • Traumatic hip dislocation • Osteoarthritis
Slipped capital femoral epiphysis (SCFE) aka "Slipped upper femoral epiphysis" is a medical term referring to slippageof the overlying epiphysis of proximal femur posteriorly and inferiorlydue to weakness of the growth plate. Most often, it develops during periods of accelerated growth, shortly after the onset of puberty.
Slipped capital femoral epiphysis .. A Klein line is a line drawn along the superior border of the femoral neck that would normally pass through a portion of the femoral head. If not, slipped capital femoral epiphysis is diagnosed. The patient's left hip (arrow) shows that a slight shift of the head of the femur occurred through the growth plate.
Slipped capital femoral epiphysis .. 1. Risk Factors • most common in the adolescentperiod (boys aged 10-16 y, girls aged 12-14 y). • Maleshave 2.4 times the risk as females. • Obesity is a risk factor because it places more shear forces around the proximal growth plate in the hip at risk. • Bilateralslippage is common (but the left hipis affected more commonly than the right).
Slipped capital femoral epiphysis .. 2. Etiology 1. Overweight 2. Endocrinedisorders (e.gadiposogenital dystrophy, primary or secondary hypothyroidism). 3. Deficiency or increase of androgens. 4. Acute trauma. Slipping of the upper femoral epiphysis occurs predominantly in obesechildren with underdeveloped sexual characteristics and less commonly, in tall, thin children.
Slipped capital femoral epiphysis .. 3. Pathology • The slip occurs in the hypertrophic zone of the growth plate. • 70% slow and progressive(This is gradual, with slowly increasing symptoms over a period of weeks or even months. In chronic slipping, there may be no history of trauma and the symptoms are often quite mild). • 30% acute due to trauma(Least common, this usually follows severe trauma such as a fall from a height ). • If the slip is sever anterior retinacular vessels are torn → avascular necrosis. • Physeal slip → premature fusion of the epiphysis within 2 years.
Slipped capital femoral epiphysis .. 4. Clinical Features 1. Pain: in the groin and around the knee. 2. Limp(intermittent). 3. Shorteningof the affected limb (1-2 cm). 4. The limb is in external rotation. 5. Flexion, abduction, medial rotation are limited. 6. External rotation, adduction are increased.
Slipped capital femoral epiphysis .. 5. Diagnosis The diagnosis is a combination of clinical suspicion plus radiological investigation. 20-50% of SCFE are missed or misdiagnosed on their first presentation to a medical facility. This is because the common symptom is knee pain. This is referred pain from the hip. The knee is investigated and found to be normal • Ultra sound : • AP X-ray :(melting ice cream cone) 1. Widening of the growth plate. 2. Trethowan’s sign : Line up superior margin of neck should intersect epiphysis (usually 20% of the femoral head lateral to this line) 3. Capeners sign : In pelvic AP view in the normal hip, the posterior acetabular margin cuts across the medial corner of the upper femoral metaphysis. With slipping, the entire metaphysis is lateral to the posterior acetabular margin • Lateral X-ray : Slip Posterior horn of the neck is lower than anterior horn.
Slipped capital femoral epiphysis .. Grading Severity of SCFE according to AP and Lateral X-ray views
Slipped capital femoral epiphysis .. It is important to determine if the lesion is stable or unstable : 1. "Stable" SCFEs allow the patient to (walk) with or without crutches (walking aids). 2. "Unstable" SCFEs do not allow the patient to ambulate at all; these cases carry a higher rate of complication, particularly of AVN.
Slipped capital femoral epiphysis .. 6. Complications 1. Avascular necrosis. 2. Chondrolysis. 3. Osteoarthritis. 4. Coxavara(is a deformity of the hip, whereby the angle between the ball and the shaft of the femur is reduced to less than 120 degrees). 5. Slipping of the opposite hip ≈ 20% of cases
Slipped capital femoral epiphysis .. NOTE : Coxa Vara a deformity of the hip, whereby the angle between the ball and the shaft of the femur is reduced to less than 120 degrees. This results in the leg being shortened, and therefore a limp occurs. It is commonly caused by injury, such as a fracture. It can also occur when the bone tissue in the neck of the femur is softer than normal, meaning it bends under the weight of the body.
Slipped capital femoral epiphysis .. 7. Treatment 1. Mild Cases : Epiphysis fixation by kirschner wires or screws 2. Severe Cases : In-situ pinning correction of the deformity by subtrochantric osteotomy
Slipped capital femoral epiphysis .. X-ray of a hip following operative percutaneous fixation of a slipped capital femoral epiphysis
Hip Dislocation(traumatic) Occurs when the head of femur slips out of its socket in the hip bone (pelvis). In approximately 90% of patients femur is pushed out of its socket posteriorly This leaves the hip in a fixed position, bent and twisted in toward the middle of the body. Femur can also slip out of its socket anteriorly the hip will be bent only slightly, and the leg will twist out and away from the middle. A hip dislocation is very painful. Patients are unable to move the leg and, if there is nerve damage, may not have any feeling in the foot or ankle area.
Traumatic Hip Dislocation .. NOTE : Hip dislocations are relatively uncommon during athletic events.Injuries to small joints (eg, finger, wrist, ankle, knee) are much more common. However, serious morbidity can be associated with hip dislocations. • Direct force trauma (minor or major force) to the thigh is the most common cause of hip dislocation. • Large force traumas (e.g motor vehicle accidents, pedestrians being struck by automobiles). This type of injury also is associated with high-energy impact athletic events (e.g American football, rugby, water skiing) Children may have a hip dislocation due to relatively minor trauma.
Traumatic Hip Dislocation .. 1. Posterior Hip Dislocation (90%) : • Posterior dislocations occur when the knee and hip are flexed and a posterior force is applied at the knee while the leg is in adducted position. • Posterior hip dislocations occur typically during RTAs, when the knees of the front-seat occupant strike the dashboard.
Traumatic Hip Dislocation .. Signs & Symptoms of Posterior Hip Dislocation : • 1. pain in the hip and buttock area. • 2. The affected limb is shortened, adducted, and internally rotated, with the hip and knee held in slight flexion. • 3. Patient may be unable to walk or adduct the leg. • 4. Signs of vascular or sciatic nerve injurymay be present : • - Pain in hip, buttock, and posterior leg • - Loss of sensation in posterior leg and foot • - Loss of dorsiflexion(peroneal branch) or plantar flexion (tibial branch) • - Loss of DTRs at the ankle. • - Local hematoma in vascular injury.
Traumatic Hip Dislocation .. Management of Posterior Hip Dislocation : • the Bigelow maneuver • may be performed with minimal assistance with the patient in the supine position . Place the patient supine on a stretcher that is elevated to the height of the waist of the practitioner performing the reduction. The injured hip is initially held in a position of adduction and internal rotation, with one practitioner applying longitudinal distraction and an assistant applying pressure on the patient's anterior superior iliac spines so as to stabilize the patient's pelvis.
Traumatic Hip Dislocation .. Management of Posterior Hip Dislocation : • Allis maneuver • Under GA, place the patient in supine position. • While an assistant stabilizes the pelvis with direct pressure, Flex the hip and knee to 90° and pulls the thigh vertically upward. Complications of Posterior Hip Dislocation : • 1. Sciatic nerve injury. • 2. Vascular injury (hematoma). • 3. Avascular necrosis. • 4. Osteoarthritis.
Traumatic Hip Dislocation .. 2. Anterior Hip Dislocation : Anterior dislocation of the hip occurs from a direct blow to the posterior aspect of the hip or, more commonly, from a force applied to an abducted leg that displace the hip anteriorly out of the acetabulum.
Traumatic Hip Dislocation .. Signs & Symptoms of Anterior Hip Dislocation : • 1. Pain in the hip area and inability to walk or adduct the leg • 2. The leg is externally rotated, abducted, and extended at the hip. • 3. The femoral head may be palpated anterior to the pelvis. • Signs of injury to the femoral nerve or artery may be present: • femoral nerve : • Paresis of lower extremity • Weak or absent DTR at knee • Paresthesias of lower extremity • femoral artery: • dull aching pain, pallor, paresthesias, and coldness.
Traumatic Hip Dislocation .. Management of Anterior Hip Dislocation : • Reduction: almost identical to post. dislocation, except while the thigh is pulled upward it should be adducted then an assistant helps by applying lateral traction to the thigh. Complications of Anterior Hip Dislocation : • Avascular necrosis. • femoral nerve injury. • femoral artery injury.
Traumatic Hip Dislocation .. 3. Central Hip Dislocation : The third type of hip dislocation is a central dislocation in which a direct impact to the lateral aspect of the hip forces the hip centrally through the acetabulum into the pelvis. This is a fracture -dislocation.
Traumatic Hip Dislocation .. Indications for Open Reduction : • 1. Irreducibledislocation • 2. Persistentinstability of the joint following reduction (e.g fracture-dislocation of the posterior acetabulum) • 3. Fractureof the femoral head or shaft • 4. Neurovasculardeficits that occur after closed reduction
Osteoarthritis Chronic degenerative disorder in which there is progressive articular hyaline cartilage destruction and new bone formation, with remodeling of joint contour. Accompanied by new cartilage and bone proliferation at the joint margins.
Osteoarthritis .. • Most common non-traumatic disorder of the hip in middle and late age. Healthy fit and over 50 years of age. • In younger patients it may appear as a sequel to acetabular dysplasia, coxa vara ,slipped epiphysis. • Secondary osteoarthritis arthritis is seen in older patients after secondary RA, avascular necrosis, or paget’s disease.
Osteoarthritis .. Pathology : Area of maximal loading (top of the joint) shows marked changes: 1. Articular cartilage becomes soft and fibrillated. 2. underlying bone shows cyst formation and sclerosis. At the margins of the joint there are the characteristic osteophytes. Synovial hypertrophy and capsular fibrosis.
Osteoarthritis .. Clinical features : 1. Pain : felt in the groin and radiates to the knee typically after periods of activity, later it becomes constant and disturbs sleep. 2. Stiffness. 3. Limping. 4. Muscle wasting. 5. Deep tenderness. 6. Restrictedmovements.
Osteoarthritis .. X – Ray : Earliest sign is a decreased joint space. Later signs are subarticular sclerosis, cyst formation and osteophytes at the edges of the joint.
Osteoarthritis .. • Osteoarthritis of the hip showing joint space narrowing at the weight bearing surface and osteophyte formation.
Osteoarthritis .. • Osteophytosis(arrow) is noted at the articular margin of the femoral head.
Osteoarthritis .. Treatment : Mainly symptomatic. 1. Analgesics. 2. Use of a walking stick. 3. Preserve movement and stability by performing exercises within the range of comfort. 4. Joint manipulation sometimes relieves pain for long periods. 5. changing life style to reduce impact loading on the affected hip e.g Climbing up and down the stairs, carrying heavy weights
Osteoarthritis .. Operative Treatment : • Indicated in : • Severe pain • Progressive decrease in joint movement • Increase difficulty with activities of daily living • X-ray signs showing progressive joint deterioration. • The procedure of choice is total hip replacement.
Osteoarthritis .. Hip Replacement : Hip replacement is a surgical procedure in which the hip joint is replaced by a prosthetic implant. Hip replacement surgery can be performed as a total replacement or a hemi (half) replacement. Such joint replacement orthopaedic surgery generally is conducted to relieve arthritis pain or fix severe physical joint damage as part of hip fracture treatment. A total hip replacement (total hip arthroplasty) consists of replacing both the acetabulum and the femoral head while hemiarthroplasty generally only replaces the femoral head. Hip replacement is currently the most successful and reliable orthopaedic operation with 97% of patients reporting improved outcome.
Bashar Tammabi7amdillah THANK YOU www.sawa2006.com Medical ppt http://hastaneciyiz.blogspot.com