Download
1 / 44
450 likes | 672 Views
Approach to the open lung biopsy, pattern analysis. Leyla MEMİŞ,M.D. University of Gazi, School of Medicine.

E N D
Approach to the open lung biopsy, pattern analysis Leyla MEMİŞ,M.D. University of Gazi, School of Medicine
Interstitial lung diseases encompass approximately 200 entities ,in which the lung is altered by a combination of interstitial inflammation, granulomatous inflammation or fibrosis. Trawis WD,Colby MN,Koss MN et all: Atlas of nontumor pathology:Non-neoplastic disorders of the lower respiratory tract.2002
An accurate diagnosis is critical to the management of patients with idiopathic interstitial pneumonia. • Kevin R. Flaherty, Talmadge E. King, Jr., Ganesh Raghu, Joseph P. Lynch, III, Thomas V. Colby, William D. Travis, Barry H. Gross, Ella A. Kazerooni, Galen B. Toews, Qi Long, Susan Murray, Vibha N. Lama, Steven E. Gay and Fernando J. Martinez • Idiopathic Interstitial Pneumonia What Is the Effect of a Multidisciplinary Approach to Diagnosis?
Diagnostic Approach • Clinical features, • High-resolution computed tomography (HRCT) • Surgical lung biopsy all play a role in establishing a diagnosis.
Chronic Interstitial Pneumonias areChronic • Typically symptoms persist more than 3-6 months • and frequently have been present for years.
Diagnostic Approach • We believe that at a minimum the evaluation of patients with idiopathic interstitial pneumonia should include an interaction between the clinician and thoracic radiologist. If this initial step results in a confident diagnosis of IPF a surgical lung biopsy is not required. • In all other cases a surgical lung biopsy is likely to impact the final diagnosis and should be performed if possible. • Kevin R. Flaherty, Talmadge E. King, Jr., Ganesh Raghu, Joseph P. Lynch, III, Thomas V. Colby, William D. Travis, Barry H. Gross, Ella A. Kazerooni, Galen B. Toews, Qi Long, Susan Murray, Vibha N. Lama, Steven E. Gay and Fernando J. Martinez • Idiopathic Interstitial Pneumonia What Is the Effect of a Multidisciplinary Approach to Diagnosis?
High-resolution computed tomography (HRCT) • Chest x-rays must show bilateral reticulonodular infiltrates . • ‘Lines and dots’ pattern • Ground glass change
bilateral reticulonodular infiltrates . • ‘Lines and dots’ pattern represent the combination of inflammation and focal parenchymal scarring.
Ground glass change reflects active interstitial disease and corresponds to aggregates of macrophages and/or fibromyxoid connective tissue in alveolar spaces.
For diagnostic surgical pathology, histologic pattern recognition is most useful and is applicable even in small biopsies. Trawis WD,Colby MN,Koss MN et all: Atlas of nontumor pathology:Non-neoplastic disorders of the lower respiratory tract.2002
Transbronchial biopsies have limited role for the diagnosis of mostdiffuse interstitial lung diseases.
Transbronchial biopsies are useful for the diagnosis of: • Sarcoidosis • Infection • Tumor • Lymphangioleiomyomatosis • Alveolar proteinosis • Amyloidosis • Eosinophilic pneumonia
Open Lung Biopsy • Don’t biopsy the lingula and right middle lobe • Don’t biopsy the very fibrotic lung • Biopsies must be large ( at least 5 cm in greatest dimention ) and deep • More than one lobe biopsy if possible
histologic pattern recognition!! pathologist pathologist
Pattern Analysis I • Diffuse:The inflammatory reaction involves all portions of the lung parenchyma. • Patchy:İnflammatory reaction only affects selected areas of the lung parenchyma
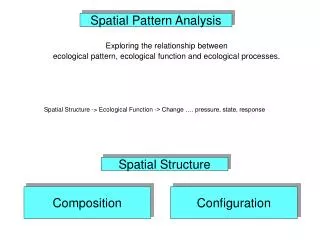
Pattern Analysis IIAnatomical Distribution • Pleural/Subpleural • Bronchocentric/bronchiolocentric • Angiocentric • Lymphatic distribution • Peripheral acinar • Septal changes (vascular changes with chronic passive congestion) • Airspace consolidation • Diffuse interstitial infiltration Colby,Lombard,Yousem,Kitaichi:Atlas of pulmonary surgical pathology.1991.
Pattern Analysis II - Anatomical Distribution Schematic anatomic illustration of lung biopsy Colby,Lombard,Yousem,Kitaichi
Subpleural/ Peripheral acinar pattern Early phase Subpleural/ Peripheral acinar pattern Late phase
Bronchocentric Mixed pattern Broncocentric pattern Luminal changes
Bronchocentric/bronchiolocentric • Respiratory bronchiolitis • Hypersensitivity pneumonitis • Giant cell interstitial pneumonia • Bronchiectasis • COP/BOOP • Small airways disease
Diffuse interstitial infiltration
Alveolar septal • Nonspecific interstitial pneumonitis • Desquamative interstitial pneumonitis • Diffuse alveolar damage,late stage • Lymphoid interstitial pneumonia
Lymphatic distribution leukemia Lymphatic distribution Sarcoidosis-Lymphoma
Lymphangitic • Lymphangitic carcinoma • Sarcoidosis • Lymphangioleiomyomatosis • Low grade lymphoma (MALT type)
Temporal homogeneity Fibrosis at same ages Temporal heterogeneity Fibrosis at different ages Pattern Analysis III(Interstitial injury pattern)
Pattern Analysis IV Reaction Patterns of the distal lung parenchyma
Reaction Patterns of the distal lung parenchyma • Diffuse alveolar damage • Diffuse alveolar hemorrhage • Organizing pneumonia pattern • Cellular interstitial infiltrates • Desquamative interstitial pneumonia-like pattern • Interstitial fibrosis • Granulomatous interstitial pneumonia • Lymphocytic interstitial pneumonia / diffuse lymphoid hyperplasia • Bronchiolar injury
Diffuse alveolar damage Diffuse alveolar hemorrhage
NSIP LIP
The separation of UIP from other non-UIP disorders is critical.
Differential Diagnosis of Chronic Interstitial Pneumonias • Acute interstitial pneumonia • Granulomatous interstitial pneumonias Sarcoidosis Hypersensitivity pneumonitis • Langerhans’ cell histiocytosis