Download
1 / 48
510 likes | 2.39k Views
Breast Pain and Nipple Discharge. Philip Turton Consultant Breast, Oncoplastic, and Aesthetic Breast Surgeon Leeds General Infirmary. Mastalgia alone or in combination with lumpiness is the commonest reason for referral to a breast clinic. Pain alone 17% Lumpiness and pain 33%

E N D
Breast Pain and Nipple Discharge Philip Turton Consultant Breast, Oncoplastic, and Aesthetic Breast Surgeon Leeds General Infirmary
Mastalgia alone or in combination with lumpinessis the commonest reason for referral to a breast clinic Pain alone 17% Lumpiness and pain 33% Non painful lump 36% Nipple discharge 5% Family history 3% 50%
Breast Pain • Theory • Imbalance of essential fatty acids • Hormonal stimulation • Endogenous sensitivity of some breast lobules • Almost never associated with malignancy with normal examination
Breast Pain Non breast mastalgia should be differentiated by a good history Consider: Angina, GS, Cervical spondylosis, Cervical rib, oesophageal erosions, lesions and achalasia, rib fracture, torn/strained muscle, pleuritic pain, pneumonia, pulmonary lesion, Tietz’s syndrome
Non-cyclical pain • Unrelated to the menstrual cycle • Described as tight, burning or sore • Constant or intermittent • Usually affects one breast, in a localized area, but may spread more diffusely across the breast • Usually affects postmenopausal women in their 40s and 50s
Cyclical Breast Pain • Clearly related to the menstrual cycle • Described as dull, heavy or aching • Often accompanied by breast swelling or lumpiness • Usually affects both breasts, UOQs, +/- radiates to axilla • Intensifies during the two weeks leading up to the start of your period, then eases up afterward • Usually affects premenopausal women in their 20s and 30s and perimenopausal women in their 40s
Mastalgia: Taking a good history Age, FH, parity Previous history of breast problems: cysts, pain, biopsies, cancer, surgery (BBA, BBR, mastopexy) Previous breast imaging- what, why and when When was last period? Menstrual irregularities Usage of OCP, depot, mirena coil, progesterone only pill
Breast Pain Assess the pain: pain chart if not straightforward Site, type, intensity, duration of symptoms frequency previous occurrence Current impact on QOL Specific concerns eg cancer
FIGURE 3.1 FIGURE 3.1 Back to Chapter 3 thumbnails Back to Contents
FIGURE 3.2 FIGURE 3.2 Back to Chapter 3 thumbnails Back to Contents
Examination NB: re-examine after next period if presenting in the week prior to menstruation
Who can be managed initially in primary care • Bilateral symmetrical cyclical pain, which resolves following menstruation • Recent onset breast pain, with normal examination in young patient • Male patients with simple tender gynaecomastia • Normal examination and recent normal breast imaging • If in doubt, please refer
Treatment Educate and Reassure Refit bra if obvious problem/ sports bra helps in short term Topical NSAID gel Avoid caffeine completely Evening primrose oil: 1gm od or BD for minimum of 3-months, with good compliance If on HRT- reduce If recently started COCP - reassure If mirena/prog only pill, consider other
Breast Pain Who to refer: “anything atypical” 1. Pain associated with definite signs: eg dominant or discrete lump, palpable focal thickening: will have triple assessment 2. Patients who have previously had breast cancer Rib met, lung met, LR 3. Persisting pain, same quadrant for 3-months Mammo + targetted USS normal or B9 changes carries almost 100% negative predictive value. Core of any focal area but is uncommon
Hospital Treatment of Severe Mastalgia • Tamoxifen 10-20mg OD, 4-months • Use on days 5 to 21 of cycle most effective • S/E hot flushes, vaginal dryness • Very rare: DVT
Treatment • Danazol 100mg tds, 4-months • Inhibits pituitary gonadotrophins (FSH & LH) • Stimulates androgenic pathways • S/E: acne, oily skin, hirsuitism, weight gain, voice change, thrombosis
Treatment • Bromocriptine 2.5mg OD, 4-months • Stimulates dopamine receptors in the brain and inhibits release of prolactin • Avoid in post-partum period (MI, CVA, HT) • S/E drowsiness, headache, postural hypotension, nausea, dizziness, dry mouth, fibrotic reactions
Treatment • GnRH analogues, • Decrease FSH/LH (after initial surge) • S/E: Hot flushes, sweating, vaginal dryness, loss of libido
Breast Pain Treatment of non-cyclical breast pain Usually as for cyclical More likely to use oral NSAID early on Often due to duct ectasia; more common after menopause Is there a chance that cancer can be present? Rare in absence of palpable thickening, or lump. Ensure breast looks & feels normal, and no obvious palp LN Repeat examination after 6-weeks
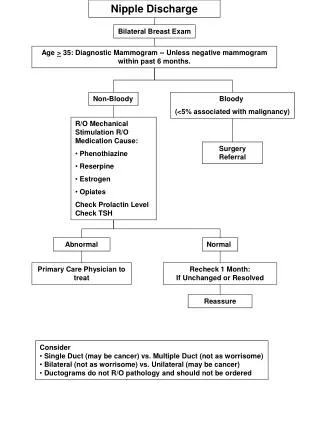
Nipple Discharge • Causes • Physiological • Duct ectasia • Mild inflammation • Post-partum • Papilloma • DCIS, Inv ca • Abscess • Very rare: endocrine cause, joggers nipple Papillomas and duct ectasia commonly arise in the sub areola segment
Duct ectasia An aberration of development & involution Women >50 Nipple discharge, retraction, doughy palpable mass Discharge cheesy/ white Slit-like nipple retraction Management conservative or surgical Surgical = total duct excision
Nipple Discharge Taking a History • When • Spontaneous, or on Squeezing • Frequency & duration • Consistency & quantity: spotting on bra, or staining through to blouse • Blood stained • Current medication: phenothiazines, haloperidol, methyldopa
Colour • Usually always insignificant: multi-duct • Brown and haem negative • Green • White, creamy • Investigate: single duct • Brown and haem negative but persistent • Brown and haem positive • Serous • Blood stained • Galactorrhea NB: Use the standard urinalysis sticks
History • Associated breast symptoms or signs • Any lump • Any changes near the NAC • Nipple inversion, nipple eczema • Adjuncts to assess risk • Parity • FH of breast or ovarian ca • Previous breast problems, abnormal breast biopsies • For galactorrhea: amenorrhea/headache/visual
Examination • Apart from the nipple discharge, examination is usually normal • Look for the rarely associated signs of a sinister cause • Indrawing, lump, sub-areola thickening
Investigation of new nipple discharge Advise to cease expression Mammogram/USS if persists Review in 2-3 months If persistent bilateral, do serum prolactin Investigate further in breast clinic
Investigation • Nipple fluid: haem test • If positive do Hadfields procedure • Nipple fluid: smear onto a slide for cytology- • Epithelium should not be seen ie should be “negative for epithelial cells” • If positive for epithelial cells indicates higher possibility of papilloma or DCIS, therefore do Hadfields procedure to send tissue to pathologist
Investigation • >35: Mammo and USS of NAC • <35: USS of NAC • Guided biopsy • Eg USS guided core or FNAC of ?intraductpapilloma • NB: Any clinically palpable lump must always be biopsied even if mammo and USS are normal
Treatment • Diagnostic Surgery • Uncommon: microdochotomy/Ductoscopy • “Hadfield’s Procedure” • Sub areola excision of the major breast ducts, which is sent for histology • S/E: nipple sensation, nipple necrosis, infection • Therapeutic operation • Where results of Hadfields procedure show DCIS/Inv ca: Usually mastectomy & IBR
Treatment of non-significant nipple discharge • Advise not to squeeze the nipple to look for further discharge • If persists and is nuisance can refer for further investigation • Would tend to do a therapeutic Hadfields • Ie the purpose is to stop the discharge with the operation instead of doing it for diagnostic assessment alone
Key Points • Breast Pain: • Most do not need referring, reassure, educate • Refer: not settling, focal nodularity, lump • Nipple Discharge: • Most are physiological or duct ectasia • Refer: watery or blood stained Handouts: please email me on eplt@aol.com Any breast related queries: philip.turton@leedsth.nhs.uk NHS secretary: Angela Mathie: 0113 3922250
Spiculate mass right breast Normal left breast
USS of Right Breast Cancer, and USS core, confirming needle through lesion
Handouts: please email me on eplt@aol.com Any breast related queries: philip.turton@leedsth.nhs.uk