Download
1 / 16
160 likes | 170 Views
Head & Cup Simulator. Why do we use simulator? To verify the accuracy of new methods.

E N D
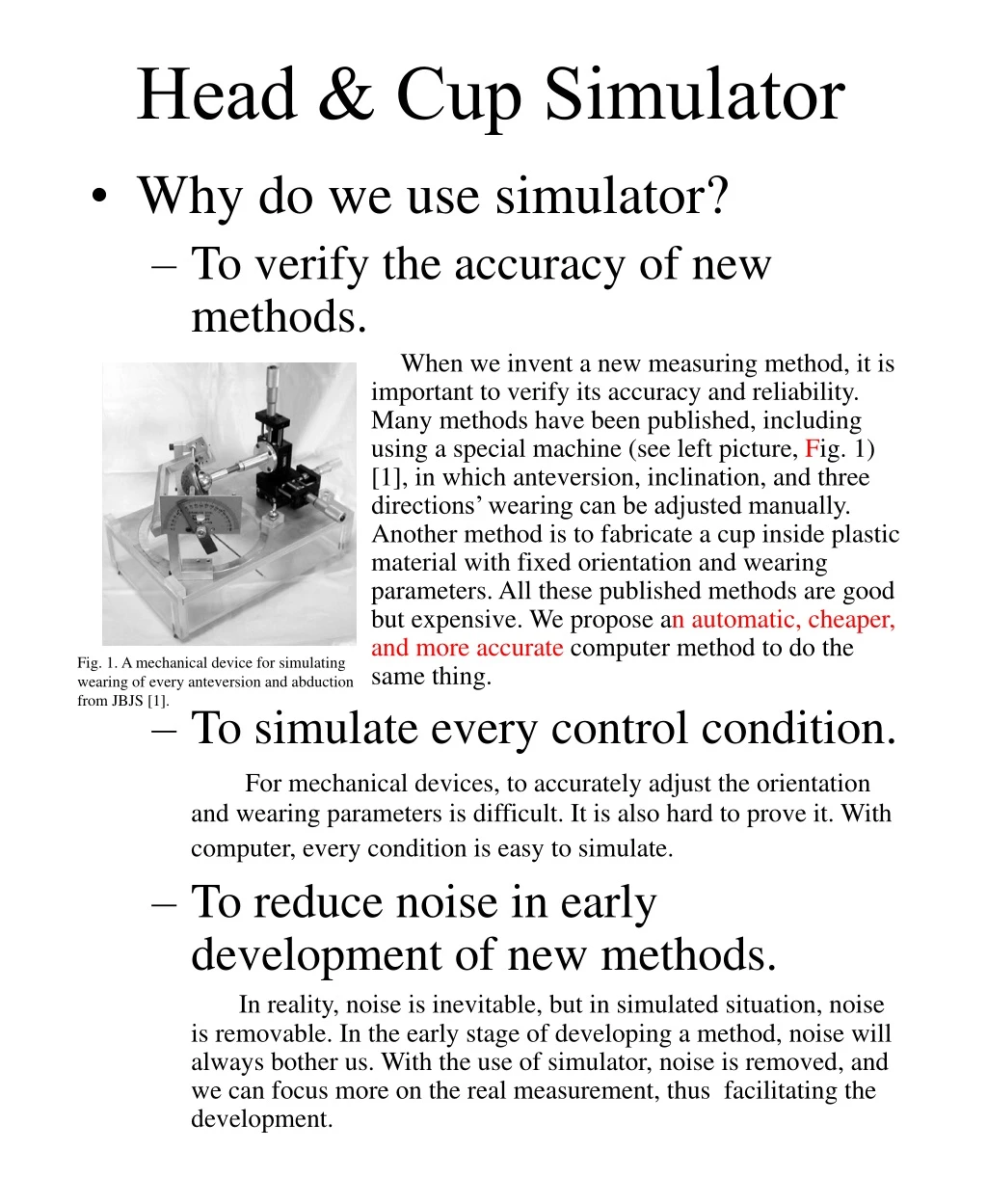
Head & Cup Simulator • Why do we use simulator? • To verify the accuracy of new methods. When we invent a new measuring method, it is important to verify its accuracy and reliability. Many methods have been published, including using a special machine (see left picture, Fig. 1) [1], in which anteversion, inclination, and three directions’ wearing can be adjusted manually. Another method is to fabricate a cup inside plastic material with fixed orientation and wearing parameters. All these published methods are good but expensive. We propose anautomatic, cheaper, and more accurate computer method to do the same thing. • To simulate every control condition. For mechanical devices, to accurately adjust the orientation and wearing parameters is difficult. It is also hard to prove it. With computer, every condition is easy to simulate. • To reduce noise in early development of new methods. In reality, noise is inevitable, but in simulated situation, noise is removable. In the early stage of developing a method, noise will always bother us. With the use of simulator, noise is removed, and we can focus more on the real measurement, thus facilitating the development. Fig. 1. A mechanical device for simulating wearing of every anteversion and abduction from JBJS [1].
How does the simulator work? • Line tracing method We simulate every X-ray beam traveling from source to the film. The simulated prosthesis projection will be calculated. The total thickness of metal is estimated and then we translate to gray level of the simulated X-ray. • Why not using OpenGL or DirectX? DirectX is the 3D tool of Windows. The OpenGL is the open source version of 3D tool. They are useful and effective in virtual reality. They are good in drawing non-transparent object. In our case, the X-ray beam is a highly penetrating radiation. We are drawing a semi-transparent object. It is hard to use OpenGL or DirectX, although they are quite good in performance. • Absorption law The X-ray is a kind of radiation beam with high energy. It follows the general rule of absorption. Beer-Lambert law: -kbcPenetration = ek: molar absorbability (a) b: path length c: concentration (b) It is hard for us to use it on our simulator. • Absorption example (Fig. 2) • Lookup table method The simulated X-ray was analyzed. We build a table with known thickness, in which we can deduce its photo-density on X-ray. We then look up the table, interpolate the data and then get the result of photo-density. Fig. 2. (a)A metal model made of titanium with 1, 2, …, 5mm thickness. (b) Its X-ray image.
PE Wear Meter • What did we do before? In the past, we measured PE wear manually. A well accepted method is Livermore’s method (Fig. 3) [2]. He finds the center of femoral head, measures the thinnest PE, and then reads the wear. • What’s new? Fig. 4a. Hardinge’s method Fig. 4b. Shaver’s method (need to point out p1, p2, p3) Fig. 4c. John’s method (need to point out ischial tuberoses). As the computer technology progresses, some digitalized methods [3][4][5] (Fig. 4) have been proposed. All of them need human hand to point out several important landmarks. With the new invention on computer vision, we propose a new method to make the computer find the prosthesis by itself and then compute. No manual intervention is needed. Fig. 3c. Then measure it. Fig. 3b. Find the thinnest polyethylene. Fig. 3a. Livermore’s method, find head center.
Our method • Find head-neck junction by cross-correlation Fig. 5. Make a template and mark corresponding head-neck junction and the indicated place. At first, we make an ordinary X-ray with template. Then we mark the important landmark and pointout the indication from it. The program will use cross-correlation method, find the corresponding landmark on the other X-rays, and then find the indicated place. This procedure is the most time-consuming procedure and costs about 60 seconds (Pentium 500MHz computer). This is also our original contribution to this method. • Project 200 lines from indicated place to upper right side with about 135 degrees span. • Detect edges with vector edge detector. Using vector edge detector subroutine, we detect the shell edges. These edges are rechecked again and again in order to remove noise such as screw or others. We consider currently published edge detectors unsuitable, so we invent a new one. It detects vectory edges, so we called it vector edge detector.
Our method (cont.) • Find center from the 200 detected edges. The center of the 40 edges are found by calculus. Then the program will exclude the extremes and find center again and again, until there are no extremes. • Project 240 lines from the new center with 270 degrees span. The lower left part is excluded. • Find head edges with the same vector edge detector. • Find the head center Again, the center of femoral head is found with exclusion of extremes. • Check centers by “Hill-Climbcing Search” [7] • Compare the two centers, and find the displacement vector. • .
Materials & Methods • Simulated data • 64 simulated X-rays with 2 different anteversion angles, 2 different abduction angles, 4 different superior wears, and 4 different medial wears. • We measure these simulated X-rays automatically by our “Auto PE Wear Meter” program. • The results are compared. • Real X-rays • We digitized 88 total hip arthroplasty X-rays using Sony S70 digital camera size (2048*1680). • The camera was set with the same distance and same zoom.
Real X-rays (Cont.) • There is no exclusion criteria of digitization. • Results classification: • Wrong detection on cross-correlation • Wrong detection of acetabulum • Wrong detection of head • Minor error on acetabular center estimation • Minor error on head center estimation • Unmeasurable X-ray by Livermore’s method • Partially measurable X-ray, which can be measured by other method • Measurable X-ray by Livermore’s method
Results • Simulated data -Our program can detect 61 of 64 simulated X-rays without misdetection (Fig. 6). -The three mis-detected X-rays images were due to misdetection of acetabulum (Fig. 7). • The error on measuring medial directional wear using our program is -0.023~+0.176mm. • The error on measuring upper wear using our program is -0.152~+0.315mm. Fig. 6. Four examples of successful detection Fig. 7. The three misdetections.
Fig. 8. Wrong detection due to cross correlation. • Real X-rays • 47 excellent detections • 2 unknown errors • 3 wrong detections on cross-correlation (Fig. 8) • 23 wrong detections of acetabulum (Fig. 9) • 3 wrong detections of head (Fig.10) • 10 minor errors on acetabular center estimation (Fig. 11) • 0 error on head center estimation • 19 unmeasurable X-rays by Livermore’s method (Fig. 12) • 49 partially measurable X-rays, which can be measured with instrument (Fig. 13) • 21 measurable X-rays by Livermore’s method (Fig. 14) Fig. 9. Wrong detection on finding acetabulum. Fig. 10. Wrong detection on finding head. Fig. 11. Minor error on fitting the circle with acetabulum edges. Fig. 12. Head-acetabulum edges are too unclear to use Livermore’s method. Fig. 13. With instrument, the thinnest edges can be detected by other edges. Fig. 14. Measurable by Livermore’s method.
Fig. 15a. Head edges are unclear to be detect manually. Fig. 15b. Our program can detect the edges and find the best fitting circle. Fig. 16a. Unmeasurable by Livermore’s method. Fig. 16b. The program can measure it. 2 X-rays measurable by program but unmeasurable manually 27 X-rays measurable by program but unmeasurable by Livermore’s method 24 X-rays measurable manually but unmeasurable by program 8 X-rays measurable by Livermore’s method but unmeasurable by program Fig. 17a. Measurable manually. Fig. 17b. Misdetection by our program. Fig. 18b Misdetection by our program. Fig. 18a. Measurable by Livermore’s method.
Discussion • In the simulated data, error in medial wear is -0.023~+0.176mm and error in upper wear is -0.152~+0.315mm. • Compared with literature [1][6], in which the error listed was 0.1mm, our method is as good as other computer-assisted methods. • Our program is the first fully automatic program in which no human intervention is needed for detection. • Detection rate: • Our program: 54.5% (40/88).If we accept minor error, the rate becomes 65.9% (58/88). • Livermore’s method: 23.9% (21/88) • Others: 78.4% (69/88)
Reasons of misdetection • Low kv As we know, the kv of X-rays will change the penetration power. When the kv is low, the penetration power is low. On the other hand, when the kv is high, the penetration power is high. If the kv is too low, the bone and prosthesis will be saturated as white. If the kv is adjusted high, the prosthesis will be whiter. That makes detection easy. • Screw noise The screws of acetabulum are located just above it. That is the place where our program detects edges for estimating acetabulum center. Sometimes, the screws cause noises and misdetections. • Bone noise The edges of bone will cause white lines on X-rays. If the white lines intersect the prosthesis edges, they may cause misdetection. • Distortion • X-ray filming When the X-rays pass through body to film, there are grids between body and film to filtrate scattering. The grids may cause torsions and make circles became ellipses. • Digitizing There are several devices for digitizing X-rays. The digital cameras take pictures through lens. The lens will cause distortion. • Validation Currently, we have not tested our program on revision hip arthroplasty, which is to measure wears after removal of polyethylene and compare it with preoperative X-rays. This should be our future work.
Conclusions • We designed a program which can automatically measure polyethylene wear. We have tested it on simulated X-rays and the result is encouraging. Clinical validation is needed in future work.
Authors • Liaw Chen-Kun, MD, Visiting Staff, Department of Orthopaedic Surgery, En Chu Kong Hospital • Wu Tai-Yin, MD, Fellow, Department of Family Medicine, Jen-Ai General Hospital • Hou Sheng-Mou, MD, Professor, Department of Orthopaedic Surgery, National Taiwan University Hospital • Yang Rong-Sen, MD, Professor, Department of Orthopaedic Surgery, National Taiwan University Hospital • Fuh Chiou-Shann, PhD., Professor, Department of Computer Science and Information Engineering, National Taiwan University • Liaw Shong-Hon, MD, Resident, Department of Emergency, Sin-Lau Christial Hospital • Wu Chang-Chin , MD, Visiting Staff, Department of Orthopaedic Surgery, En Chu Kong Hospital • Tai Han-Cheng , MD, Visiting Staff, Department of Orthopaedic Surgery, En Chu Kong Hospital • Liu Dah-Hsiang , MD, Visiting Staff, Department of Orthopaedic Surgery, En Chu Kong Hospital
Institutions • En Chu Kong Hospital • National Taiwan University Hospital • Department of Computer Science and Information Engineering, National Taiwan University
Reference • Ebramzadeh E, Sangiorgio SN, Lattuada F, Kang JS, Chiesa R, McKellop HA, Dorr LD. Accuracy of measurement of polyethylene wear with use of radiographs of total hip replacements. [Journal Article] Journal of Bone & JointSurgery - AmericanVolume. 2003;85-A(12):2378-84. • Livermore J, Ilstrup D, Morrey B. Effect of femoral head size on wear of the polyethylene acetabular component. J Bone Joint Surg Am. 1990;72:518-28. • Hardinge K, Porter ML, Jones PR, Hukins DW, Taylor CJ. Measurement of hip prostheses using image analysis. The maxima hip technique. J Bone Joint Surg Br. 1991;73:724-8. • Shaver SM, Brown TD, Hillis SL, Callaghan JJ. Digital edge-detection measurement of polyethylene wear after total hip arthroplasty. J Bone Joint Surg Am. 1997;79:690-700. • Martell JM, Berdia S. Determination of polyethylene wear in total hip replacements with use of digital radiographs. J Bone Joint Surg Am. 1997;79:1635-41. • Collier MB. Kraay MJ. Rimnac CM. Goldberg VM. Evaluation of contemporary software methods used to quantify polyethylene wear after total hip arthroplasty. [Evaluation Studies. Journal Article] Journal of Bone & JointSurgery - AmericanVolume. 85-A(12):2410-8, 2003 Dec. • Stuart R. Peter N. Artificial Intelligence A Modern Approach. [book] 111-114.
