Download
1 / 9
100 likes | 320 Views
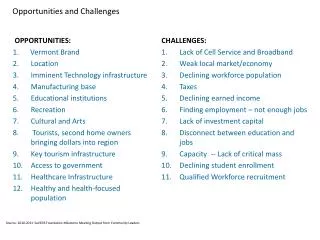
Overview of Challenges and Opportunities. The Affordable Care Act (ACA) presents many challenges and opportunities for the community mental health center providers in Indiana.

E N D
Overview of Challenges and Opportunities The Affordable Care Act (ACA) presents many challenges and opportunities for the community mental health center providers in Indiana. The healthcare home model is being aggressively developed by various states as an opportunity to pursue an effective method of providing treatment for individuals with chronic disease. Under Section 2703 of the Affordable Care Act, opportunities exist for states to improve care for Medicaid enrollees with chronic health conditions, including serious mental illness, by providing federal funding for comprehensive care management and coordination, as well as health education and promotion activities. Under the healthcare home model specific standards have been developed to ensure specific individuals with chronic conditions have access to this improved service delivery approach. The standards include; 1) Medicaid beneficiaries with two or more chronic conditions (mental health, substance abuse, asthma, diabetes, heart disease, being overweight) 2) One chronic condition and at risk for a second; 3) a Serious and persistent mental health condition; 4) Dual eligibles cannot be excluded; and 5) Can serve individuals within a subset of specific chronic conditions.
Overview of Challenges and Opportunities Community mental health providers in Indiana must be prepared for this changing dynamic since the healthcare home model include the behavioral health consumers currently being treating within the CMHC system. This approach also requires the consideration of newly eligibles who will meet this definition. Such consumers are high utilizers of both primary and behavioral health services due to the nature of the illness and the impact on overall well-being. The expanding the pool of eligible Medicaid recipients will most certainly mean that an increase in the number of individuals pursuing access to behavioral health services will occur in the CMHC system in Indiana. As the healthcare home model is gaining momentum as a way of effectively delivering care in the context of chronic disease, it becomes critical that executive teams within the CMHC system work in collaboration with state Medicaid policy makers to design a healthcare home model that considers cost effective service delivery for individuals with chronic mental illness.
Overview of Challenges and Opportunities The ICCMHC was a member of the an E-Learning Action Community that was developed through the National Council and focused on the ability of Indiana and other participating states to prepare for the new health eco-system. This approach required an extensive analysis of both providers and state Medicaid to prepare and adjust to this new system for delivering healthcare in Indiana. Through this extensive “readiness” process, the participating members of the team developed a “Rapid Cycle Change Plan” which attempts to prepare community mental health centers providers of the changes in healthcare delivery with a focus on the delivery of services for those with chronic and persistent mental illness. A large part of the Indiana Council’s initiative over the next year is to further develop this plan, in cooperation with participating members, to develop a blueprint for each CMHC to use in the development of the skills, resources, and training required to carry out these new provisions. This in large part is the basis for today’s meeting, which is not seen as a continual “preaching” about the changing healthcare environment, but rather a working meeting, where participating members contribute to the plan’s developed based on the previously identified goals from the Rapid Cycle Change Plan as developed by the committee.
Overview of Challenges and Opportunities The primary goals of the Rapid Cycle Change Plan include; GOAL # 1: Develop Health Home and/or ACO Partnerships. GOAL # 2: Rapid Reengineering of Key Agency Activities to Prepare for the new Healthcare Ecosystem. GOAL # 3: Pursue effective integration of primary and behavioral healthcare through initial partnerships while developing the required competencies to delivery primary healthcare within behavioral healthcare environment. Over the coming year, developing a plan to address each of these goals will be the primary focus of the Indiana Council and the membership. In light of a changing political landscape, completing this plan over the next several months will position the CMHC system to carry out the goals and objectives of the ACA, while ensuring that community mental health services are the primary vehicle for chronic mental health consumers.
Overview of Challenges and Opportunities The current Daniels Administration is in its final year of existence, which means our focus is on positioning ourselves for new state leadership. Regardless of whether the new administration is Republican or Democrat, it is important the CMHC system in Indiana demonstrates our ability to improve health outcomes for chronic mental health consumers while reducing Medicaid costs. Such an approach requires not only a plan of action, but also health outcome data which can be used to demonstrate how investing in services delivery within the CMHC for individuals with chronic mental health conditions will lower Medicaid costs. Using an already CMS approved model for home health service delivery , the Community Mental Health Center system in Indiana must provide evidence that WE ARE the effective method, with the appropriate workforce, and the infrastructure to carry out these important ACA provisions. This approach requires that we rely on the current and effective leadership of our CMHC CEOs and executive management teams to design, define, and demonstrate our capabilities.
Overview of Challenges and Opportunities By working collaboratively, we jointly envision how the integrated care and healthcare home model should look in Indiana for people living with serious mental illnesses within the context of allowable Medicaid services delivered in a more cost effective fashion. The Healthcare home model is comprised of six services including; 1) Comprehensive care management; 2) care coordination and health promotion; 3) comprehensive transitional care/follow-up; 4) patient and family support; 5) referral to community and social support services; and 6) the use of health information technologies to link services. Typically goals for healthcare homes include enhancing access to coverage and services, improving health quality and reducing racial and ethnic disparities, integrating care for people with complex and special needs; and building Medicaid capacity to address the expected increase in the number of individuals having access to services.
Overview of Challenges and Opportunities By working collaboratively the CMHC system and state Medicaid we can focus on improved health outcomes, reduced emergency room visits, hospitalizations, readmissions, and reliance on long-term care facilities. The ability to determine cost effectiveness is largely dependent on the development of health outcome data that documents the costs savings to the overall healthcare system through coordinated care. Indiana Medicaid providers must aggressively examining health outcome data from health organizations throughout the country in order to determine cost effective health service delivery for behavioral health consumers suffering from chronic disease. This requires a new examination of current data collection processes. As Section 2703 of the Affordable Care Act creates opportunities for states to improve care for Medicaid enrollees with chronic health conditions, including serious mental illness, by providing federal funding for comprehensive care management and coordination, as well as health education and promotion activities it becomes important that the State of Indiana consider this changing dynamic.
Overview of Challenges and Opportunities Under this section, the state can amend its Medicaid state plans to create Healthcare Homes with improved federal financial participation. States such as Missouri have already submitted and had their SPA approved to include a behavioral healthcare home. Such states are taking advantage of improve federal matching participation rates which lessons the financial burden on states. We know that we cannot effectively meet the behavioral needs of consumers if we ignore the fact that individuals with SMI, on average die 25 years earlier than the general population, and that 60% of these premature deaths are due to medical conditions, such as cardiovascular disease and pulmonary and infectious diseases that are either going undiagnosed or untreated. In addition, we know that our own treatment approaches can contribute to high risk health condition as second generation anti-psychotic medications are highly associated with weight gain, diabetes, abnormal cholesterol levels and metabolic syndrome. We also know that treating mental illness is not enough. Wellness and prevention are as important as treatment and rehabilitation. And in order to truly improve outcomes and the quality of life for the individuals we serve, we have to focus more attention on the general health care problems that interfere with recovery.
Overview of Challenges and Opportunities As there is continuing pressure to find new ways to control state Medicaid costs, it becomes more important than ever that CMHC executives and state Medicaid policy leaders assist work collaboratively in this effort by confirming the value of community mental health center services in the treatment of individuals suffering from chronic health conditions. CMS will require that Indiana measures its success by tracking and reporting outcomes (i.e., avoidable readmissions, emergency room visits, and skilled nursing facility admissions) and calculate cost savings. Designated providers must report quality measures as condition of reimbursement. Health teams (Section 3502 of ACA) must also report patient outcomes and experience. Considering willingness of CMHC providers, in collaboration with health outcome data researchers to assist in the required health quality outcome data process, Indiana could be better positioned than other states to pursue this opportunity under the ACA. Now is the time for effective leadership within our organization, and today is simply the start of a year long process that will ultimately secure the role of the CMHC system in Indiana as the best and most appropriate choice for treating chronic mental health disorders under the new healthcare eco-system.