Download
1 / 27
280 likes | 503 Views
Mass Home Care ’ s 2012 Network Conference. Community Care Linkages SM A Division of Mass Home Care. September 11, 2012. Topics. Implementation of ACA New Models of Care and Payment Reform Community Care Linkages Year 2 The COMMUNITY LIVING Program Next Steps.

E N D
Mass Home Care’s 2012 Network Conference Community CareLinkagesSMA Division of Mass Home Care September 11, 2012
Topics • Implementation of ACA • New Models of Care and Payment Reform • Community Care Linkages Year 2 • The COMMUNITY LIVING Program • Next Steps
Health Care Delivery System Transformation Acute Health Care System 1.0 Coordinated Seamless Health Care System 2.0 Community Integrated Health Care System 3.0 • High quality acute care • Accountable care systems • Shared financial risk • Case management and preventive care systems • Population-based quality and cost performance • Population-based health outcomes • Care system integration with community health resources
Innovation Center Portfolio Primary Care Transformation • Comprehensive Primary Care Initiative (CPC) • Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration • Federally Qualified Health Center (FQHC) Advanced Primary Care Practice Demonstration • Independence at Home Demonstration ACOs • Medicare Shared Savings Program • Pioneer ACO Model • Advance Payment ACO Model • PGP Transition Demonstration Bundled Payment for Care Improvement • Model1: Retrospective Acute Care • Model 2: Retrospective Acute Care Episode & Post Acute • Model 3: Retrospective Post Acute Care • Model 4: Prospective Acute Care • Capacity to Spread Innovation • Partnership for Patients • Community-Based Care Transitions • Million Hearts • Innovation Advisors Program • Health Care Innovation Challenge Initiatives Focused on the Medicaid Population • Medicaid Emergency Psychiatric Demonstration • Medicaid Incentives for Prevention of Chronic Diseases • Strong Start Initiative • Dual Eligible Beneficiaries • State Demonstration to Integrate Care for Dual Eligible Individuals • Financial Models to Support State Efforts to Integrate Care • Demonstration to Reduce Avoidable Hospitalizations of Nursing Facility Residents
Health Care’s BLIND SIDEThe Overlooked Connection between Social Needs and Good Health Robert Wood Johnson Foundation summary reviews key findings from an online survey of 1,000 American physicians in the American Medical Masterfile who agreed to be invited to participate in the survey. The participation rate was 5 percent (1,000 physicians completed the survey out of 20,000 invited to participate); 690 were primary care physicians and 310 were pediatricians. • 85% physicians surveyed say unmet social needs are directly leading to worse health. • 85% physicians surveyed say patients’ needs are as important to address as their medical conditions. • Especially true (more than 9 in 10, or 95%) for patients in low-income, urban communities. • 76% would like the health care system to cover the costs associated with connecting patients to services that meet their social needs; and • 80% are not confident in their capacity to address their patients' social needs.
Health Care’s BLIND SIDE Con’t http://community.rwjf.org/community/healthcaresblindside • Top social needs they would write a prescription for include: • Fitness program 75% • Nutritional food 64% • Transportation assistance 47% • For patients in mostly urban and low-income communities • Employment assistance 52% • Adult education 49% • Housing assistance 43%
Bridging medical care and long term services and supports (LTSS) is a critical component to meeting the needs of individuals with chronic conditions and functional limitations, and improving system outcomes. Riskbearing entities present a unique avenue to pursue this integrated vision.
Aging Network – An Infrastructure that Supports 11 Million Older Adults and Caregivers AoA 56 State Units on Aging 629 Area Agencies 246 Tribal organization 20,000 Service Providers & 500,000 Volunteers Provides Services & Supports to 1 in 5 Seniors 242 million meals 28 million rides 29 million hours of personal care 69,000 caregivers trained 855,000 assisted 4 million hours of case management 0ver 22,000 individuals transitioned 81,759 individuals completing CDSMP
ASAP Strategy: Link Primary Care to Community Home Care Services • Getting to: • High quality acute care • Accountable care systems • Shared financial risk • Case management and preventive care systems • Population-based quality and cost performance • Population-based health outcomes • Care system integration with community health resources Community Integrated Health Care System 3.0 Community CareLinkagesSMA Division of Mass Home Care Achieve triple aim objectives by linking primary care practices to community care management services • Reduce costs through prevention and/or reduction of unnecessary utilization of health care services • Improve health outcomes through better care coordination and patient education • Improve patient experience and satisfaction by aligning with goal of remaining functionally active at home
Pioneer ACOs • Experienced in coordinating care across all care settings • Allow rapid movement from a shared savings payment model to a population-based model • Separate track from Medicare Shared Savings Program • Coordinated with private payers to align provider incentive to achieve triple aim CMMI selected 32 in US, 5 in MA: • Atrius Health • Beth Israel Deaconess Physician Organization • Mount Auburn Cambridge Independent Practice Association (MACIPA) • Partners Healthcare • Steward Health Care System
Medicare Shared Savings/ Advanced Payment ACOs Circle Health Alliance, LLC , Lowell Comprised of partnerships between hospitals and ACO professionals, with 353 physicians. It will serve Medicare beneficiaries in Massachusetts and New Hampshire. Coastal Medical, Inc. (Providence, RI) ACO group practices, with 100 physicians to serve Medicare beneficiaries in Massachusetts and Rhode Island Jordan Community ACO, Plymouth • 100+ physicians from Plymouth Bay Medical Associates, Jordan Physician Associates, and a number of specialty physicians from Jordan Hospital to coordinate the healthcare of 6,000 Medicare beneficiaries in Plymouth and Barnstable Counties. Physicians of Cape Cod ACO • Physicians of Cape Cod ACO to serve approximately 5,000 beneficiaries living in Cape Cod, Massachusetts. Harbor Medical Associates PC, South Weymouth • ACO group practices, with 116 physicians, to serve Medicare beneficiaries in Massachusetts.
Integrated Care Entities (ICOs)for Dual Eligibles Primary Care Independent LTSS Coordinator ICO will be required to contract with community-based organizations to provide independent LTSS Coordinators LTSS Coordinator must have no financial interest in the determination of an enrollee’s type or amount of services LTSS Coordinator is a member of the care team, at the enrollee’s discretion After initial assessment, if enrollee has specific needs outside the designated LTSS Coordinator’s expertise, ICO will arrange for assignment of a more appropriate LTSS Coordinator LTSS Coordinator will work with enrollee to incorporate community-based services as appropriate into care plan • Primary care and behavioral health will be integrated • All members will choose a provider • Primary care providers may be at varying levels of capability to perform as person-centered medical homes (PCMHs); ICOs are ultimately accountable for all care, and must support primary care providers to become medical homes and/or Health Homes
Community Care Linkages Community Care Linkages is a strategic initiative to effectively integrate services of the Massachusetts Aging Services Access Points (ASAPs) into the evolving healthcare delivery system. Who are the MA ASAPs? • 27 Not-for-Profit Organizations • A 35 year old statewide network linking community resources to individuals and their families • Managing 70,000 covered lives annually in home care programs (~$340m of services across MA) • Bring value to evolving community based health care systems. www.Communitycarelinkages.org www.masshomecare.org
MEMBER-CENTERED LONG TERM SERVICES & SUPPORTS FOR DUAL ELIGIBLES The COMMUNITY LIVING Program • Statewide network • Successful partnering with community agencies and medical providers • ILCs, ADRCs, SCOs, ACOs • Key Services • Initial Assessment • Basic Coordination • Complex Care Coordination • RN Assessments • Network Management • Evidenced-Based Healthy Living Programs A Mass Home Care Initiative for Integrated Care Organizations
Community-based Care Transitions Program (CCTP) 47 partners announced in three rounds, 4 in Massachusetts • Elder Services of Berkshire County • Berkshire Medical Center and the Berkshire Visiting Nurse Association • Elder Services of Worcester & BayPath Elder Services • MetroWest Medical Center; St. Vincent Hospital; UMass Memorial Medical Center; Wing Memorial Hospital; Marlborough Hospital; Clinton Hospital, and HealthAlliance Hospital • Somerville-Cambridge Elder Services & Mystic Valley Elder Services • Cambridge Health Alliance and Hallmark Health System • Merrimack Valley of Massachusetts and Southern New Hampshire Elder Services • Anna Jacques Hospital, Saints Medical Center, Holy Family Hospital, Lawrence General Hospital, and Merrimack Valley Hospital http://innovation.cms.gov/initiatives/Partnership-for-Patients/CCTP/partners.html
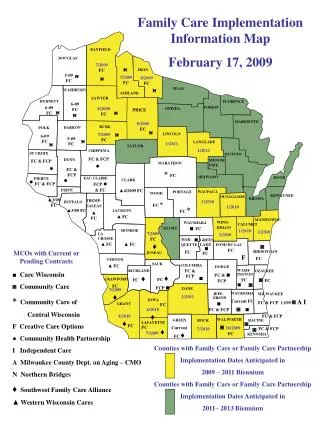
FY11 ASAP Spending ~$340m On Behalf of MA Executive Office of Elder Affairs
Many Partnering Initiatives Underway • Physicians: • Acton Medical • Atrius Health • Family Practice Group • HCA (BIDMC) • Lahey Medical Group • Meeting House Family Practice • The Medical Group • Somerville Primary Care Selected Partners Activities Services: Dedicated Link CTI/Enhanced Coleman Community Liaison On-site Options Counseling Meetings: Inpatient interdisciplinary team STAAR Teams PCMH Multi Payer Initiative Continuum of Care Quality Assurance Initiative Emergency Dept. CMS CMP Community Connections Group Hospitals: • Baystate Health System • Berkshire Medical Center • BIDMC • Brockton • Cambridge • Cooley Dickinson • Emerson Hospital • Health Alliance • Gardner • Lahey Clinic • Milford Regional • Partners Healthcare • Northeast Health System • Steward Norwood Hospital • Tufts Medical Center • UMass Medical Center • Vanguard Health Systems • Winchester
Hospital/ASAP Collaboration “Emerson Hospital and Minuteman Senior Services have banded together with the goal of preventing unnecessary repeat hospital stays.”
Atrius Health/ASAPs Practice-Based Pilots • Chelmsford & Elder Services of Merrimack Valley • Peabody & North Shore Elder Services • Southboro & Baypath • West Roxbury & Ethos • Concord & Minuteman Senior Services • Watertown & Springwell Currently expanding to new sites Community CareLinkagesSMA Division of Mass Home Care
Atrius Health 100% on an electronic medical record combined with corporate data warehouse, used for managing quality and cost. Long history with global payments: greater than 50% of patients under global risk across Commercial, Medicare and Medicaid Widespread use of rosters in population management Track record of quality measurement and reporting Over 30 NCQA certified Level 3 Patient-Centered Medical Homes
Why Pioneer? “Reason for Action” Participating in the Pioneer ACO will help Atrius Health achieve high-quality, high-value care for all Medicare-eligible patients across the care continuum. Successful implementation for Medicare-eligibles will improve performance for commercial risk patients with similar clinical needs. Access to full claims data set for Pioneer population offers true opportunity to be accountable for quality and cost across the continuum. Contracting for Medicare Fee for Service patients under a global budget through Pioneer ACO maintains our position as a market leader in payment reform, moving towards 100% global payment.
Atrius Health – ASAP Collaboration Community CareLinkagesSMA Division of Mass Home Care • Expansion of the “Care Team” to include the patient’s home and community-based networks • Requires: effective communication for timely and efficient referrals, hand offs, and “closing the loop” • Results in: patient centered care plans with realistic goals and resources for implementation • Collaboration through: • Practice-based Pilots • Population-based Interventions
Atrius Health – ASAP Practice-based Pilot Community CareLinkagesSMA Division of Mass Home Care • Practice referral to ASAP with brief description of patient/needs • Referral form completed and faxed along with the problem list, medication list and the latest office visit • ASAP contacts the patient and arrange an intake interview, updating practice on barriers and services recommended • ASAP provides services, closes the loop with practice via phone call • Practice documents care coordination note and routes to PCP pool. Epic flag notes patient receiving care from ASAP.
Population-Based Intervention:Falls Risk Assessment Community CareLinkagesSMA Division of Mass Home Care • Identify population appropriate for home-based FRA • Develop standard work for non-medical ASAP intervention (population based, rather than practice or ASAP dependent) • Develop data capture in Epic to meet Pioneer quality measure
Current ASAP/ACO Contracts Atrius Health/Southboro Medical Group (SMG) & BayPath for “Community Social Services” • Social Worker from BayPath to support SMG 24 hours per week • Access to SMG EpicCare (EHR) • Provide general community social services • Participate in case management, quality assurance and quality improvement, utilization review and peer review activities • Metrics: • Number of patients referred • Number of ED admissions • Number of hospital readmissions • Pre- and post-intervention costs • Number of cases on-going • Number of resistant patients referred – must define non-compliant
“one woman I&R department” Current ASAP/ACO Contracts Beth Israel Deaconess Physician Organization (BIDPO)/ Springwell for “Community Care Linkages” • a Springwell-employed Community Resource Coordinator (CRC) to work on site at BIDPO’s office located in Westwood, MA, 3 days per week • identify the most affordable community resource options available to meet the identified needs of any referred Patient regardless of age or ASAP eligibility • educate the BIDPO’s CNCMs and other staff as to range of community resources available, including the abilities of ASAPs, so that CNCMs are fully aware of potential supports available to Patients • identify ASAP clients receiving services by any of the 27 ASAPs in MA and work with BIDPO staff to identify additional services that may be helpful to Patients who are receiving services from a Massachusetts ASAP • establish a community resources catalogue or reference library • participate with BIDPO staff in case conferences • Options Counseling visits
Next Steps Expand partnering opportunities Share learnings from 4 Care Transitions (CCTP) projects Prepare for ICO LTSS coordination opportunity Develop “The COMMUNITY LIVING Program” for all providers/payers Successfully contract with healthcare providers and payers under new health reform models Continue to share best practices and support ASAP collaborative efforts