Download

1 / 59
740 likes | 1.58k Views
Anti VEGF. Options in the management of CNV. 1) Observation occult CNV also requires close follow – up .every 3 month 2) Laser coagulation 3) Surgery 4) Triamcinolone 5) Anti angiogenic drugs (lucentice,Avastin) 6) PDT & TTT 7) Diet rich antioxidants

E N D
Options in the management of CNV 1)Observation occult CNV also requires close follow – up .every 3 month 2) Laser coagulation 3) Surgery 4) Triamcinolone 5) Anti angiogenic drugs (lucentice,Avastin) 6) PDT & TTT 7) Diet rich antioxidants with severe AMD) .(217 cases)
Used for: Wet Macular degeneration Diabetic retinopathy 3) Rubeosis iridis 4) CRVO
VEGF and diabetic eye disease 1)Diabetic retinopathy remains the major cause of blindness in working – eye adults in the world.
2) It appears to be different retinopathy phenotype and many eyes may remain with minimal retinopathy changes and good vision for an entire lifetime.
Inhibition of the enzyme PK- C (proteinkinas-c) (angiogenesis factor) with ruboxistaurin represents a particularly exciting therapeutic approach it works at the early stages of the diabetic retinal disease when the disease is still reversible.
(Intravitreal) Steroids Have been used with some success in advanced situations of chronic diffuse diabetic macular edema. Are effective only in the short term and are associated with complications such as cataract and glaucoma.
The combination of intravitreal steroid with laser therapy has been shown is another interesting alternative.
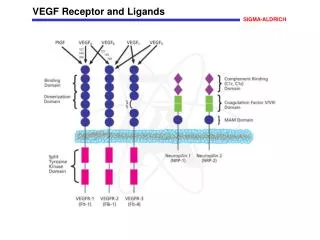
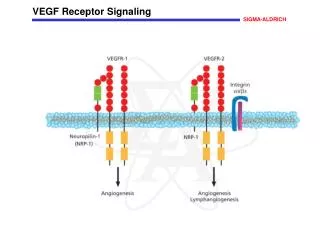
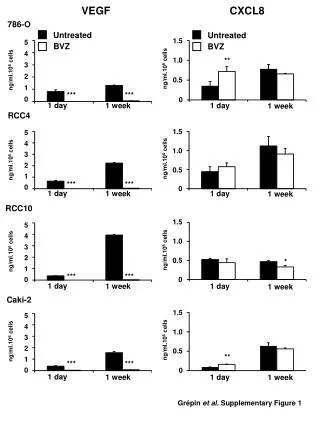
VEGF An increase in VEGF (vasoendothelial growth factor) has been repeatedly demonstrated in the vitreous of advanced case of diabetic retinopathy
VEGF INHIBITORS 1)(Avastin) Bevacizumab. 2)(Macugen) or pegaptanib sodium. 3)(lucentis) or Ranibizumab
Avastin costs less than 150 $ Per treatment compared with 2000$ per treatment for lucentis.
Anti-VEGF Freeman: Anecdotaly the Anti _ VEGF drugs have proven. Very useful in treating proliferative diabetic retinopathy.
Anti-VEGF It is proven that is effective in wet macular degeneration and there is a growing consensus that this will be true in diabetes and retinal vascular disease.
Avastin or Lucentis 1) Reduce macular edema in diabetic pts. 2) Reduce or stop proliferative retinopathy
The big problem with these drugs is that they have to be given on an on going basis These drugs don't cure any thing. They reduce VEGF
Anti VEGF When the drug wears off the patients need injections every four to six weeks.
Challenge The challenge is to deliver these drugs in away that would suppress VEGF chronically we don't know how to do this yet.
Kenalog(Triamcinolone) and anti- VEGF causes actual vision improvement.
Laser + subtenon injection of Kenalog (steroid) stabilize the vision.
Stabilize the vision If you stabilize vision when patient is still at 20/30 that patient is going to do better than someone in whom the diagnosis is delayed and vision is worse.
Laser problem Loosing peripheral and night vision
Treated patients 1) Showed better visual acuity 2) Greater reductions in retinal thickness 3) Reduced need for PRP 4) Regression of Neovascularization 5) Microaneurysms and hemorrhage improvement
Bevacizumab (Avastin) is in clinical trial for treatment of diabetic macular edema and retinopathy at centers in IRAN , Mexico & Venezuela
Ruboxistaurin is a drug that is administered in tablet form and also produced promising early results. However, it is now uncertain whether Eli Lilly will continue to develop the drug, following a recent FDA decision mandatimy three years of additional clinical trials.
Remote diabetic retinopathy screening by: 1)Digital imaging 2) Non-mydriatic exams. 3) Internet