Download
1 / 50
500 likes | 532 Views
THALASSEMIAS. A WIDE VARIETY of diseases involving GLOBIN synthesis, COMPLEX genetics Alpha or beta chains deficient synthesis involved Often termed MAJOR or MINOR, depending on severity, silent carriers and “ traits ” are seen

E N D
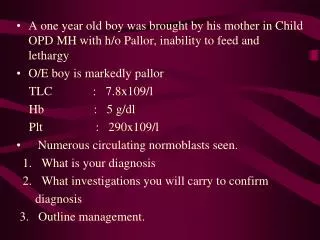
THALASSEMIAS • A WIDE VARIETY of diseases involving GLOBIN synthesis, COMPLEX genetics • Alpha or beta chains deficient synthesis involved • Often termed MAJOR or MINOR, depending on severity, silent carriers and “traits” are seen • HEMOLYSIS is uniformly a feature, and microcytic anemia, i.e, LOW MCV (just like iron deficiency anemia has a low MCV) • A “crew cut” skull x-ray appearance may beseen in severe erythroid hyperplasia.
Hemoglobin H Disease • Deletion of THREE alpha chain genes • HGB-H is primarilly Asian • HGB-H has a HIGH affinity for oxygen • HGB-H is unstable and therefore has classical hemolytic behavior
HYDROPS FETALIS • FOUR alpha chain genes are deleted, so this is the MOST SEVERE form of thalassemia • Many/most never make it to term • Children born will have a SEVERE hemolytic anemia as in the erythroblastosis fetalis of Rh disease: • Pallor (as in all anemias), jaundice, kernicterus • Edema (hence the name “hydrops”) • Massive hepatosplenomegaly (hemolysis)
Paroxysmal Nocturnal Hemoglobinuria (PNH) • ACQUIRED, NOT INHERITED like all the previous hemolytic anemias were • ACQUIRED mutations in phosphatidylinositol glycan A (PIGA) • Note: It is “P” and “N” only 25% of the time! GlycosylphosPhatidylInositol (lipid rafts)
Immunohemolytic Anemia • All of these have the presence of antibodies and/or compliment present on RBC surfaces • NOT all are AUTOimmune, some are caused by drugs • Antibodies can be • WARM (IgG) • COLDAGGLUTININ (IgM) • COLD HEMOLYSIN (paroxysmal) (IgG)
IMMUNOHEMOLYTIC ANEMIAS • WARM AGGLUTININS (IgG), will NOT agglutinate at room temp • Primary Idiopathic (most common) • Secondary (Tumors, especially leuk/lymph, drugs) • COLD AGGLUTININS: (IgM), WILL agglutinate at room temp • Mycoplasma pneumoniae, HIV, mononucleosis • COLD HEMOLYSINS: (IgG) Cold Paroxysmal Hemoglobinuria, hemo-LYSIS in body, ALSO often follows mycoplasma pneumoniae
COOMBSTEST • DIRECT: Patient’s CELLS are tested for surface Ab’s • INDIRECT: Patient’s SERUM is tested for Ab’s.
HEMOLYSIS/HEMOLYTIC ANEMIAS DUE TO RBC TRAUMA • Mechanical heart valves breaking RBC’s • MICROANGIOPATHIES: • TTP • Hemolytic Uremic Syndrome
NON-Hemolytic Anemias:i.e., DE-creased Production • “Megaloblastic” Anemias B12 Deficiency (Pernicious Anemia) Folate Deficiency • Iron Deficiency • Anemia of Chronic Disease • Aplastic Anemia • “Pure” Red Cell Aplasia • OTHER forms of Marrow Failure
MEGALOBLASTIC ANEMIAS • Differentiating megaloblasts (marrow) from macrocytes (peripheral smear, MCV>94) • Impaired DNA synthesis • For all practical purposes, also called the anemias of B12 and FOLATE deficiency • Often VERY hyperplastic/hypercellular marrow
Vit-B12 Physiology • Oral ingestion • Combines with INTRINSIC FACTOR in the gastric mucosa • Absorbed in the terminal ileum • DEFECTS at ANY of these sites can produce a MEGALOBLASTIC anemia
ALL megaloblastic anemias are also MACROCYTIC (MCV>94 or MCV~100), and that not only are the RBC’s BIG and hyperplastic/hypercellular, but so are the neutrophils, and neutrophilic precursors in the bone marrow too, and even more so, HYPERSEGMENTED!!!
PERNICIOUS ANEMIA • MEGALOBLASTIC anemia • LEUKOPENIA and HYPERSEGS • JAUNDICE • NEUROLOGIC posterolateral spinal tracts • ACHLORHYDRIA • Can’t absorb B12 • LOW serum B12 • Flunk Schilling test, i.e., can’t absorb B12, using a radioactive tracer
FOLATE DEFICIENCY MEGALOBLASTIC AMEMIAS • Decreased Intake: diet, infancy • Impaired Absorption: intestinal disease • DRUGS: anticonvulsants, BCPs, CHEMO • Increased Loss: Hemodialysis • Increased Requirement: Pregnancy, infancy • Impaired Usage
Fe Deficiency Anemia • Due to increased loss or decreased ingestion, almost always, nowadays, increased loss is the reason • Microcytic (low MCV), Hypochromic (low MCHC) • THE ONLY WAY WE CAN LOSE IRON IS BY LOSING BLOOD, because FE is recycled!
Fe Transferrin Ferritin (GREAT test) Hemosiderin
Clinical Fe-Defic-Anemia • Adult men: GI Blood Loss • PRE menopausal women: menorrhagia • POST menopausal women: GI Blood Loss
2 BEST lab tests: • Serum Ferritin • Prussian blue hemosiderin stain of marrow (also called an “iron” stain)
Anemia of Chronic Disease* • CHRONIC INFECTIONS • CHRONIC IMMUNE DISORDERS • NEOPLASMS • LIVER, KIDNEY failure * Please remember these patients may very very much look like iron deficiency anemia, BUT, they have ABUNDANT STAINABLE HEMOSIDERIN in the marrow!
APLASTIC ANEMIAS • ALMOST ALWAYS involve platelet and WBC suppression as well • Some are idiopathic, but MOST are related to drugs, radiation • FANCONI’s ANEMIA is the only one that is inherited, and NOT acquired • Act at STEM CELL level, except for “pure” red cell aplasia
APLASTIC ANEMIAS • CHLORAMPHENICOL • OTHER ANTIBIOTICS • CHEMO • INSECTICIDES • VIRUSES • EBV • HEPATITIS
MYELOPHTHISIC ANEMIAS • Are anemias caused by metastatic tumor cells replacing the bone marrow extensively
POLYCYTHEMIA • Relative (e.g., hemoconcentration) • Absolute • POLYCYTHEMIA VERA(Primary) (LOW EPO) • POLYCYTHEMIA (Secondary) (HIGH EPO) • HIGH ALTITUDE • EPO TUMORS • EPO “Doping”
P. VERA • A “myeloproliferative” disease • ALL cell lines are increased, not just RBCs
BLEEDING DISORDERS(aka, Hemorrhagic “DIATHESES”) • Blood vessel wall abnormalities √ • Reduced platelets √ • Decreased platelet function √ • Abnormal clotting factors √ • DIC (Disseminated INTRA-vascular Coagulation), also has ↓ plats.
VESSEL WALL ABNORMALITIES(angiopathic thrombocytopenias)(NON-thrombotic cytopenic purpuras) • Infections, especially, meningococcemia, and rickettsia • Drug reactions causing a leukocytoclastic vasculitis • Scurvy, Ehlers-Danlos, Cushing syndrome • Henoch-Schönlein purpura (mesangial IgA deposits too) • Hereditary hemorrhagic telangiectasia (Osler–Weber–Rendu syndrome, Autosomal Dominant) • Amyloid
THROMBOCYTOPENIAS • Like RBCs: • DE-creased production • IN-creased destruction • Sequestration (Hypersplenism) • Dilutional • Normal value 150K-300K
DE-CREASED PRODUCTION • APLASTIC ANEMIA • ACUTE LEUKEMIAS • ALCOHOL, THIAZIDES, CHEMO • MEASLES, HIV • MEGALOBLASTIC ANEMIAS • MYELODYSPLASTIC SYNDROMES (PRE-Leukemias)
IN-CREASED DESTRUCTION • AUTOIMMUNE (ITP) • POST-TRANSFUSION (NEONATAL) • QUINIDINE, HEPARIN, SULFA • MONO, HIV • DIC, “CONSUMPTIVE” • TTP/HUS • “MICROANGIOPATHIC”
THROMBOCYTOPENIAS • ITP (Idiopathic Thrombocytopenic Purpura) • Acute Immune • DRUG-induced • HIV associated • TTP, Hemolytic Uremic Syndrome
I.T.P. • ADULTS AND ELDERLY • ACUTE OR CHRONIC • AUTO-IMMUNE • ANTI-PLATELET ANTIBODIES PRESENT • INCREASED MARROW MEGAKARYOCYTES • Rx: STEROIDS
ACUTE ITP • CHILDREN • Follows a VIRAL illness (~ 2 weeks) • ALSO have anti-platelet antibodies • Platelets usually return to normal in a few months
DRUGS • Quinine • Quinidine • Sulfonamide antibiotics • HEPARIN
HIV • BOTH DE-creased production AND IN-creased destruction factors are present
Thrombotic Microangiopathies • BOTH are very SERIOUS CONDITIONS with a HIGH mortality: • TTP (THROMBOTIC THROMBOCYTOPENIC PURPURA) • H.U.S. (HEMOLYTIC UREMIC SYNDROME) • These can also be called “consumptive” coagulopathies, just like a DIC
“QUALITATIVE” platelet disorders • Mostly congenital (genetic): • Bernard-Soulier syndrome (Glycoprotein-1-b deficiency) • Glanzmann’s thrombasthenia (Glyc.-IIB/IIIA deficiency) • Storage pool disorders, i.e., platelets mis-function AFTER they degranulate • ACQUIRED: ASPIRIN, ASPIRIN, ASPIRIN
BLEEDING DISORDERS due toCLOTTING FACTOR DEFICIENCIES • NOT spontaneous, but following surgery or trauma • ALL factor deficiencies are possible • Factor VIII and IX both are the classic X-linked recessive hemophilias, A and B, respectively • ACQUIRED disorders often due to Vitamin-K deficiencies (II, VII, IX, X) • von Willebrand disease the most common, 1%
vonWillebrand Disease • 1% prevalence, most common bleeding disorder • Spontaneous and wound bleeding • Usually autosomal dominant • Gazillions of variants, genetics even more complex • Prolonged BLEEDING TIME, NL platelet count • vWF is von Willebrand Factor, which complexes with Factor VIII, it is the von Willebrand Factor which is defective in von Willebrand disease • Usually BOTH platelet and FactorVIII-vWF disorders are present
PTT PT/INR
HEMOPHILIA A • The “classic” HEMOPHILIA • Factor VIII decreased • Co-factor of Factor IX to activate Factor X • Sex-linked recessive • Hemorrhage usually NOT spontaneous • Wide variety of severities • Prolonged PTT (intrinsic) only • Rx: Recombinant Factor VIII
HEMOPHILIA B • The “Christmas” HEMOPHILIA • Factor IX decreased • Sex-linked recessive • Hemorrhage usually NOT spontaneous • Wide variety of severities • Prolonged PTT (intrinsic) only • Rx: Recombinant Factor IX
DIC, Disseminated INTRA-vascular, Coagulation • ENDOTHELIAL INJURY • WIDESPREAD FIBRIN DEPOSITION • HIGH MORTALITY • ALL MAJOR ORGANS COMMONLY INVOLVED
DIC, Disseminated INTRA-vascular, Coagulation • Extremely SERIOUS condition • NOT a disease in itself but secondary to many conditions • Obstetric: MAJOR OB complications, toxemia, sepsis, abruption • Infections: Gm-, meningococcemia, RMSF, fungi, Malaria • Many neoplasms, acute promyelocytic leukemia • Massive tissue injury: trauma, burns, surgery • “Consumptive”coagulopathy
Common Coagulation TESTS • PTT (intrinsic) • PT INR (extrinsic) • Platelet count, aggregation • Bleeding Time, so EASY to do • Fibrinogen • Factor Assays
RBC LAB http://www.chronolab.com/hematology/2_1.htm