Download
1 / 36
360 likes | 473 Views
Diametrical Alterations of the great saphenous vein in correlation to venous reflux. By: Andre Sanchez Presented on: 04/19/12. Glossary/Table of Contents. Slide 1-Title Page Slide 2-Glossary Slide 3-About Me Slide 4- Problem Slide 5-Hypothesis Slide 6-9- Research Slide 10-Purpose

E N D
Diametrical Alterations of the great saphenous vein in correlation to venous reflux By: Andre Sanchez Presented on: 04/19/12
Glossary/Table of Contents Slide 1-Title Page Slide 2-Glossary Slide 3-About Me Slide 4- Problem Slide 5-Hypothesis Slide 6-9- Research Slide 10-Purpose Slide 11-Materials Slide 12-13-Procedure Slide 14- General Medical Survey Slide 15-16- Experimentation Slide 17-18- Venous Reflux Tests Slide 19-23- Data & Graphs Slide 24-26- Statistical Analysis Slide 27-29- Significant Discoveries Slide 30-33- Discussion Slide 34- Potential Application Slide 35-36 Bibliography
About Me As I progress in the field of science, I can’t help but feel intrigued. The emotions one undergoes when he or she makes a substantial difference in a life through scientific applications is truly unbelievable. Being only a sophomore with a strong thirst for science, I have had the life-changing opportunity to better familiarize myself with the field of medicine. With a field so diverse and vital in our world, I, like any other with a dream, have been striving to my fullest extent to reach my goals. And with this in mind, I never gave up. I decided to enroll myself in my school’s medical academy and eventually became the president of my school’s HOSA (Health Occupations Students of America) club. Not only was I blessed with this opportunity, but I was given the opportunity to experience a real-life medical occupation as a part-time employee at a local cardiovascular & vein clinic. All I had in mind was to give back to those in need. And that I did. I immediately developed a stronger taste for answers in such a field and decided to study a complex disease known as venous reflux, which many individuals suffer from each year. And to this day, I continue to love science with every new question and every new discovery.
Problem • Do the diametrical alterations of the great saphenous vein correlate with levels of venous reflux? Does venous reflux vary with differentiation of general medical measurements including time of day, age, and gender? • Independent Variables- General medical characteristics (age, gender, time, weight, height, blood pressure, leg size, physical activity); diameter change in relation to venous reflux. • Dependent Variables- Diameter change & venous reflux. • Control Variables- Human population, vascular ultrasound machine(Philips HDI 5000), 7.5mHz transducer.
Hypotheses • If the diametrical alterations of the great saphenous vein are compared in different age groups, then as age increases, venous reflux increases. • If general medical characteristics are compared with levels of venous reflux, then as BMI, blood pressure, weight, age, leg size, and great saphenous vein (GSV) diameter size increases, so will the levels of venous reflux. • If male and females are compared with levels of venous reflux, then the females will have the greater levels of reflux.
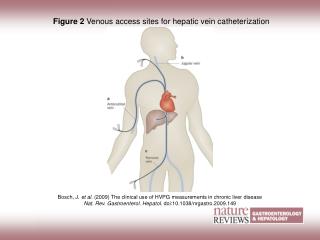
Research Within the lower extremities of the body(legs and groin area), there lies a complex set of venous junctions and networks, including the saphenofemoral junction that is home to the superficial veins of the body; the great saphenous vein and the small saphenous vein (which braches below it; linking with the femoral vein). The great saphenous vein (GSV), the longest vein in the body, stretching from the ankle to the groin region of each leg, allows blood to reach much of the lower extremities and drains into the femoral vein; near the lower abdomen and upper thigh (Hoehn et al 2010). Veins, including the GSV, have the capabilities to expand and contract throughout the day to control blood flow; however, when a vein has been stressed it tends to allow back flow of the blood, commonly known as venous reflux (Society of Interventional Radiology 2011). Venous reflux within the leg can lead to venous insufficiency or varicose veins. These varicosities are “leaking veins/valves” and do not operate properly due to the lack valve closure among the veins within the lower extremity.
Research Varicose veins can be cosmetically unappealing for manly people who have them because they leave a distinct bulge or coloration due to the vessels being swollen. These insufficient veins can also be very uncomfortable or painful, which could ultimately lead to skin ulceration or sores because they hinder the blood circulation throughout the leg. According to Cleveland Clinic (2011), each year 500,000 to 600,000 people in the United States suffer from venous ulcers and ultimately account for 80-90 percent of all leg ulcers. These skin ulcers or sores can become harmful or severe if left untreated. According to the Society of Interventional Radiology (2011), varicose veins affect 1 out of 2 people age 50 and older, and 15 to 25% of all adults. Some contributing factors include age, family history, gender, and pregnancy (Society of Interventional Radiology 2011). The GSV is prone to venous reflux due to the commonalities of venous reflux occurring in this vessel. Some symptoms associated with venous insufficiency and varicose veins in the GSV include leg pain and heaviness, which tend to worsen as the day progresses (Society of Interventional Radiology 2011).
Research According to Weiss et al (2001), the presence of visible varicose veins is typically not a reliable indicator of the extent of venous reflux within the leg. This fact is the very reason why many phlebologists use ultrasound technology to obtain a more thorough understanding. Venous reflux can be treated in a variety of manners. Treatment can be anything as simple as a change in lifestyle to schlerotherapy. Patients also have the choice to undergo vein stripping or litigation, which may be painful for patients. Within recent decades, many patients have chosen laser treatment for venous reflux, which is relatively less painful. Ultrasound imaging is a pain-free noninvasive medical test that helps physicians observe blood vessels and other internal organs. With the advancement of ultrasound technology, one can further investigate the location of blood vessels, along with their size, shape and consistency. This process is similar to that of a bat’s echolocation; since the area being observed is subjected to sound waves that allow the medical personnel to take the necessary measurements.
Research • The transducer allows the operator to focus on smaller regions of the body. The operator can manipulate the transducer to view a different image of the same area. For example, the transversal view or horizontal position of the transducer allows its operator to view a vessel and measure the diameters more accurately. However, a vertically-elongated position of the transducer allows the operator to observe the blood flow within the vessel, which is needed for the venous reflux assessment.
Purpose • The purpose of this experiment was to determine what factors contribute to venous reflux disease to develop a better understanding upon the concept of this disease. I hope scientists around the world can use this data to potentially devise an alternative treatment of venous reflux disease.
Materials • General Medical Survey • Scale with height grid • Manual Sphygmomanometer with stethoscope • Tape Measure • Philips HDI 5000 Vascular UltrasoundMachine with corresponding equipment • SG Hypoallergenic ultrasound scanning gel • Ultrasound Transducer 7.5 MHz • A Supervising Professional • A human population of both genders
Procedure 1. Provide potential subjects informed consent, if required by IRB.2. Have a trained professional supervise all activities and act as an assistant.3. Complete the necessary measurements as indicated on the survey; and record (however, allow supervisor to take blood pressure while having patient stand and be sure to wipe equipment off between subjects).4. Have the participant stand in the upright position, relaxed with bare skin of legs (from above the knee down to foot) uncovered.5. Divide legs in zones (zone 1: the knee, zone 2: mid calf, zone 3: ankle6. Apply the ultrasound scanning gel on the ultrasound transducer and on leg in all three zones. 7. Turn off lights to optimize the clarity of the lighted monitor screen of the ultrasound machine.8. Allow the assistant to place the transducer against the patient’s inner leg while you locate great saphenous vein on monitor.
Procedure 9. Freeze image and take the actual measurement of the diameter of the great saphenous vein in each zone of the leg and record values on survey.10. Allow the assistant to perform the venous reflux test by squeezing the leg just beneath the zone that is being observed and then letting go.11. Having the assistant keep the transducer on that part of leg, observe the monitor for signs of back flow and record the length of time of reflux.12. Wipe patients leg off and allow them to wash off ultrasound scanning gel.13. Allow participant to take home survey to record physical activity of the day (after morning measurements) and then allow participant to bring the survey back to be used in the evening measurement.14. Complete this procedure in the morning and then again in the evening for each participant on the same day for both legs.
Experimentation GSV Diameter Measurement through Doppler Ultrasound
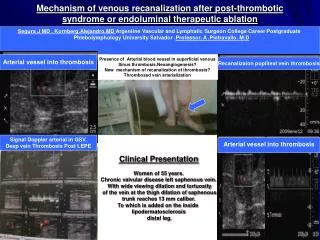
Experimentation Pulsated view of GSV-Venous Reflux Test through Duplex Scanning
Venous Reflux Test This test is known as a color-based venous reflux test using Doppler ultrasound that shows only the flow of blood along with the vessel. If you peer closely in the video, you may be able to locate the great saphenous vein (it’s the dark oval within the leg). To locate the GSV, one has to train his/her eye to find the saphenous fascia, which is the deep, connective tissue layer surrounding the vein (the whitish entity surrounding the GSV). To determine if any venous reflux exists, one must observe the change of color on the monitor; the blue is the initial squeeze or pressure that the operator does and the following red indicated a back flow of blood, otherwise known as venous reflux.
Venous Reflux Test This test is known as the pulsated venous reflux test using duplex scanning since it displays both the vessel and the pulse or levels of back flow. To complete this examination, the operator must locate the GSV in a horizontal positioning of the transducer and then gradually shift into a vertically, elongated position to stretch the scope of the vessel. The operator must then shift the angle of the machine to view within the GSV alone. In the video, the initial feedback is the pressure the operator administers and then the following spike indicated backflow (if greater than .5 seconds). So in this case, this patient had about one second of venous reflux (time it takes for the blood to return).
Data & Graphs I measured the circumference of each zone of the leg and correlated their size with that of total venous reflux throughout the day to determine if there were any significant relationships. As displayed in the graphs, all 3 regions of the leg display a positive correlation with venous reflux levels.
Statistical Analysis For this experimentation I used inferential statistics to find significant result among my data. I used t-tests to compare the average vein diameters of the morning and evening, z-score to compare females and males in proportion, and Pearson Product Moment Correlation coefficient to determine relationships within the data.
Significant Discoveries Women VS Men with Venous Reflux- Claim: Females will show greater evidence of venous reflux.Null: Both males and females will have the same amount of venous reflux.z=2.309 cv=1.960Decision: Reject Null Vein Alteration- Claim: The great saphenous vein diameter will increase throughout the day in comparison to morning measurements.Null: The great saphenous vein diameter will remain the same throughout the day. t= 4.960 cv=2.00Decision: Reject Null Age- Claim: The older participants will have higher levels of venous reflux. Null: All age groups will have the same levels of venous reflux. t=4.427 cv=4.303 Decision: Reject Null
Significant Discoveries Expanded Vessels in Evening & Venous Reflux- Claim: The expanded vessels in the evening will have the best relationship between venous reflux.Null: All vessels throughout the day will have the same amount of venous reflux. r=.850 cv=.754 Decision: Reject Null Calf Circumference & Venous Reflux- Claim: Calf size will have the greatest relation to higher levels of venous reflux. Null: All regions of the leg will equally have the same amount of venous reflux.r=.779cv=.754 Decision: Reject Null Systolic Pressure & Total Venous Reflux- Claim: Systolic pressure will have the best relationship between total venous reflux.Null: Systolic pressure will have no relation to total venous reflux. r=.808 cv=.754Decision: Reject Null
Significant Discoveries Height & Venous Reflux in the Morning- Claim: Height will correlate best to venous reflux in the morning. Null: Height will correlate to venous reflux equally throughout the day. r=.768 cv=.754Decision: Reject Null BMI & Venous Reflux in the Evening- Claim: BMI will best correlate to venous reflux in the evening.Null: BMI will correlate to venous reflux equally throughout the day. r=.765 cv=.754Decision: Reject Null Venous Reflux in Morning & Venous Reflux P.M- Claim: Venous reflux will correlate to levels of venous reflux in the evening.Null: Venous reflux in the morning will not correlate with any levels of venous reflux in the evening. t=2.325 cv=2.145Decision: Reject Null
Discussion • The data did support the claim for gender. The data was collected from 32 participants through ultrasound technology and duplex scanning. The data was then separated into two populations for analysis; those with evidence of venous reflux and those without venous reflux. Eighty-six percent of the population of venous reflux was female, whereas 14% of the population was male. There was a significant relationship between the proportion of males to females of the venous reflux population. Based on this data, I can conclude that females are more prone to have venous reflux. • The data did support the claim for vein alterations. Of the 32 subjects, the majority of the participants proved to have altering vein diameters (in expansion) in comparison to that of the morning diameters. The largest difference was 2.9mm, whereas the smallest contraction was -.6mm. Based on the data, I can conclude that compared to the morning diameters, evening diameters are significantly larger. • The data did support the claim for age. Of the venous reflux population, the older populations had the greatest levels of venous reflux with the highest average of 1.75 seconds, whereas the youth had the lowest with .5 seconds. There was a significant relationship between age and reflux. Based on this data, I can conclude that as age increases, so do the levels of venous reflux.
Discussion • The data did support the claim for expanded vessels in the evening and total levels of venous reflux. Of the venous reflux population, the largest vein diameter in the evening was 4.55mm and the highest level of venous reflux was 3.5 seconds. There was significant relationship between expanded vessels (p.m diameters) and levels of venous reflux. Based on the data, I can conclude that expanded vessels correlate with levels of venous reflux. • The data did support the claim for calf circumference and venous reflux. Of the venous reflux population, the largest calf circumference was 40.2cm and the largest amount of venous reflux was 3.5 seconds. There was a significant relationship between calf size and levels of venous reflux. Based on this data, I can conclude that calf circumference correlates with levels of venous reflux.
Discussion • The data did support the claim for systolic pressure and total venous reflux. Of the venous reflux population, the highest systolic pressure was 142mmHg with venous reflux levels of 3.5 seconds, whereas the lowest was 105mmHg with .5 seconds of venous reflux. There was a significant relationship between systolic pressure and venous reflux levels. Based on this data, I can conclude that blood pressure (systolic pressure) is a contributing factor of venous reflux. • The data did support the claim for height and venous reflux levels in the morning. Of the venous reflux population, the tallest height was 180.34cm and the largest amount of venous reflux in the morning was 1.5 seconds of back flow. There was a significant relationship between height and venous reflux levels in the A.M. Based on this data, I can conclude that height correlates with levels of venous reflux in the A.M.
Discussion • The data did support the claim for BMI and venous reflux in the evening. Of the venous reflux population, 34.33% was the greatest BMI with 3.5 seconds of venous reflux. There was a significant relationship between BMI and venous reflux in the evening. Based on this data, I can conclude that BMI is a contributing factor of venous reflux. • The data did support the claim for venous reflux in the morning compared to venous reflux in the evening. Of the venous reflux population, the largest amount of venous reflux in the morning was 1.5 seconds, whereas the largest amount of venous reflux in the evening was 2.5 seconds(solely one leg). There was a significant comparison between venous reflux in the morning and higher amounts in the evening. Based on this data, I can conclude that venous reflux levels typically increase throughout the day and are greatest in the evening.
Potential Application • I hope to use the data I have found to potentially develop an alternative treatment of venous reflux in future years (based primarily on stabilizing vein diameter changes, while permitting the flow of blood without constraint). Also, scientists can use this information to better understand this disease in the adolescents, which is relatively rare.
Bibliography Bergan, JJB. 2007. The Vein Book. Elsevier Academic Press. San Diego. 511-513. Cleveland Clinic.2011.Diseases &Conditions:Lower Extremity (Leg and Foot) Ulcers. http://my.clevelandclinic.org/heart/disorders/vascular/legfootulcer.aspx. Accessed: January 8th, 2012 Hoehn, K and EN Marieb.2010.Human Anatomy & Physiology Eighth Edition. Pearson Education, Inc. San Francisco, 701, 744 Society for Science & the Public. 2011. Intel International Science & Engineering Fair. International Rules and Guidelines 2012. SSP, Washington DC. 3-9, 17-22, 30
Bibliography Society of International Radiology 2011.Varicose and Venous Insufficiency. http:// www.sirweb.org/patient/varicose-veins/ Accessed: September 15th, 2011 Radiological Society of North America, Inc 2010, March 15.Vascular Ultrasound. http:// www.radiologyinfo.org/eninfo.cfm?pg=vascularus. Accessed: September 15th, 2011 United States. Department of Health and Human Services. Title 45 Public Welfare: Part 46 Protection of Human Subjects. Washington DC:Government Printing Office. Washington DC. Weiss, RA and CF; Feied, and MA; Weiss 2001. Vein diagnosis & treatment: A comprehensive approach. McGraw-Hill Companies, Inc. New York. 3