Download
1 / 70
710 likes | 911 Views
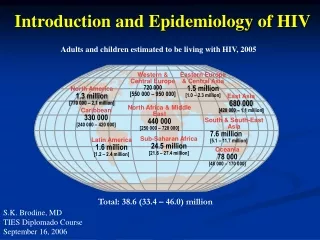
Introduction to HIV. AIM. Epidemiology Testing for HIV infection Natural history of disease When to start ART (guidelines/trends in the field) Antiretroviral agents Common toxicities Opportunistic infections OI prophylaxis. Global summary of the AIDS epidemic, 2008.

E N D
AIM • Epidemiology • Testing for HIV infection • Natural history of disease • When to start ART (guidelines/trends in the field) • Antiretroviral agents • Common toxicities • Opportunistic infections • OI prophylaxis
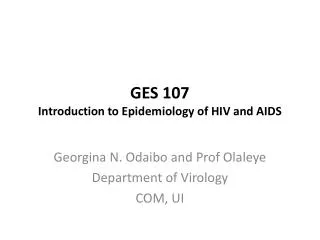
Global summary of the AIDS epidemic, 2008 Total 33.4 million [31.1 – 35.8] Adults 31.3 million [29.2 – 33.7] Women (aged 15 and above) 15.7 million [14.2 – 17.2] Children under 15 years 2.1 million [1.2 – 2.9] Total 2.7 million [2.4 – 3.0]Adults 2.3 million [2.0 – 2.5]Children under 15 years 430 000 [240 K – 610K] Total 2.0 million [1.7 – 2.4]Adults 1.7 million [1.4 – 2.1]Children under 15 years 280 000 [150 K – 410 K] Number of people living with HIV in 2008 People newly infected with HIV in 2008 AIDS-related deaths in 2008
Case • 23-year old woman presents to Emergency Department with one week history of fever, malaise, myalgias, headache and sore throat • Five days PTA she noted the onset of a new non-pruritic rash, on her face, torso, extremities • Two days PTA developed mouth sores that were so painful she was unable to eat or drink • PMH- negative • Soc Hx- sexually active, single, in grad school
Case • Physical Examination in ED T 40oC. BP 104/76 P 108 R 20 Appears unwell HEENT: Multiple oral ulcerations Non-exudative pharyngitis Multiple cervical nodes (slightly tender) Diffuse maculopapular Rash
Case • Laboratory data in ED • H/H 12/36 • WBC 3100 (65 segs, 25 lymphs, 6 atyp lymphs, 4 monos) • Platelets 71,000 • ALT 124, AST 75 • Urine drug screen negative • All other labs normal
Differential Diagnosis • Infectious Mononucleosis • CMV • HIV • Enterovirus- Coxsackie • Adenovirus • Streptococcal pharyngitis • Arcanobacterium hemolyticum • Syphilis
Principles of testing • HIV infected patients produce antibodies which recognize HIV proteins • ELISA • Western Blot • Immunofluorescence • Radioimmunoprecipitation
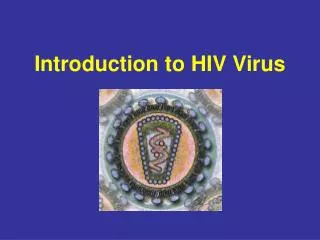
Figure 6 Proteins Detected by HIV Western Blot rev tat pol 5’ 3’ IN PRO RT R U5 U3 R p24 p17 vif env gp120 env gp41 vpu nef vpr gag HIV-1 HIV-2 }gp160/120{ }gp135/120ENV{ p61POL p61POL p55GAG p55GAG p51POL p51POL gp41ENV gp36ENV p31POL p31POL p30GAG p24GAG p18GAG p17GAG
Interpretation of Western Blot • Positive: ANY Two: p24, gp41, gp160/120 • Negative: NO positive bands • Indeterminate: the remainder • Isolated p24 band most common indeterminate • Isolated gp160/120 band suspicious for early infection
A 38 year old multiparous nurse is evaluated because of an abnormal ELISA for HIV when she attempted to donate blood. A follow up Western Blot analysis has an indeterminate result. The patient is asymptomatic. She and her husband have a monogamous relationship and neither have used illicit drugs. Patient has never received a blood transfusion, and reports a needle stick injury approximately 8 years ago from an HIV negative individual. Her physical examination is normal, her CD4 count is normal, but her plasma viral load is 82 copies/ml. Which of the following is the most appropriate management at this time? • Recheck the plasma viral load now • Recheck the HIV serologic study in 3 months and 6 months • Begin HAART • Begin HAART if her CD4 count drops to <350/µL
WB Interpretation • Infections (HIV-2 , HTLV-I, schisto) • Neoplasms • Dialysis • Ethnicity-Africans • Thyroiditis • Elevated Bilirubin • Rheumatologic diseases • Multiple pregnancy • Immunization (Tetanus, HIV) • Nephrotic proteinuria (massive) • Error in laboratory • Window period • Common variable immunodeficiency • NOT Subtype • Newest assays should identify even O Indeterminate False Negative
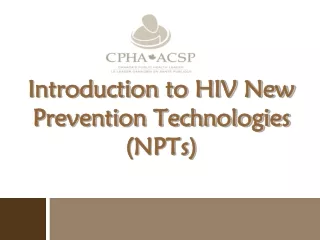
HIV Infection Profile rev tat pol 5’ 3’ IN PRO RT R U5 U3 R p24 p17 vif env gp120 env gp41 vpu nef vpr gag Anti-Env antibody Relative Level HIV RNA Detection limit P24 antigen Time Post-Infection
Natural history of the disease • Seroconversion- Median time from exposure to antibody-63 days (4 -10 wks) • Clinical latent period • Average rate of decline of CD4 cells after 1 yr is 50 cells (range- 30-90)- correlated with the viral load • PGL • Early symptomatic HIV infection • AIDS
HIV Transmission Factors • Stage of the disease • Viral load • STD • Genital lesions • Frequency of unprotected sex • Circumcision
Case • A 35 year old asymptomatic male with a CD4 count of 325, viral load of 15,000 presents to the clinic for routine evaluation. Hepatitis testing reveals that the patient has a positive HBsAg, AST-80 and ALT of 85. Which of the following is the most appropriate ART regimen • Delay treatment till he is symptomatic • Begin azt/3tc/efv • Begin abc/3tc/efv • Begin tfv/ftc/efv
Response To Therapy • Potency of antiretroviral therapy • Lower viral load • Higher CD4 count • Rapid reduction in plasma viral load in response to therapy • Approximately 70% achieve this goal and 80% of patients in clinical trial settings achieve this goal
Indications to start ART CD4 BASED IRRESPECTIVE OF CD4 COUNT History of an AIDS defining illness HIV associated nephropathy Concomitant hep B with indications to initiate hep B treatment Pregnancy • ART is recommended for patients with CD4 counts between 350 and 500 • 50% of the panel members would start ART in patients with CD4 counts greater than 500
Life Cycle of HIV Furtado MR et al. NEJM 1999;340:1614-22.
Life Cycle of HIV Maturation inhibitors Fusion Inhibitor CCR5 INHIBITORS PI NRTI NNRTI INTEGRASE INHIBITORS Furtado MR et al. NEJM 1999;340:1614-22.
Current Antiretroviral Medications Fusion inhibitor • Enfurtivide Integrase inhibitor • Raltegravir CCR5 inhibitor • Maraviroc NRTI • Abacavir • Didanosine • Emtricitabine • Lamivudine • Stavudine • Zidovudine • Zalcitabine • Tenofovir NNRTI First • Delavirdine • Efavirenz • Nevirapine Second • Etravirine PI • Amprenavir • Fosamprenavir • Atazanavir • Indinavir • Lopinavir • Nelfinavir • Ritonavir • Saquinavir • soft gel • hard gel • Tipranavir • Darunavir
Drugs in the pipeline • NNRTI inhibitors • Rilpivirine • Integrase inhibitors • Elvitegravir • CCR5 inhibitors • Vicriviroc • CXCR4 inhibitors • Maturation inhibitors • CD4 blockers
Initial Treatment: Preferred Components NRTI NNRTI • Efavirenz • Tenofovir • Emtricitabine PI • Boosted Atazanavir • Boosted Darunavir INTEGRASE • Raltegravir
Initial Treatment: Alternative Components NRTI NNRTI • Nevirapine • Abacavir • Zidovudine • Lamuvidine PI • Lopinavir/Ritonavir • Boosted Fosamprenavir • Boosted Saquinavir
Drugs with activity against hepatitis B and HIV activity • Tenofovir • Emtricitabine • Lamuvidine • Entecavir
NRTI • Toxicities • Bone marrow toxicity, macrocytic anemia, neutropeniaGI-nausea, vomiting-AZT • General-headache, insomnia, asthenia-AZT • Lactic acidosis-D4T>DDI>AZT>TFV/ABC • Pancreatitis-DDI& D4T • Peripheral neuropathy-DDI/D4T>AZT>TFV • Lipoatrophy/lipodystrophy-D4T • Myopathy (including cardiomyopathy)-AZT • Hyperlipidemia-D4T>AZT>TFV/ABC • Rapidly progressive ascending muscle weakness-D4T
NRTI • Abacavir • Abacavir hypersensitivity reaction • Fever, Rash • HLA type association with abacavir hypersensitivity • CAD • Tenofovir • Fanconi syndrome • Renal insufficiency • Dosage adjustment for Crcl<50 • Bone abnormalities in monkeys and ?fetal risks • ? osteopenia
Non-Nucleoside Reverse Transcriptase inhibitors (NNRTI) • Efavirenz • CNS toxicity • Rash • Teratogenicity • False positive cannabinoid reaction • Nevirapine • Hepatotoxicity • Highest risk in women whose CD4 count was greater than 250 at the time of NVP initiation (11.0% vs 0.9%) • Men with CD4 counts greater than 400 (6.3%vs 1.2%) • Rash, with reports of TEN and SJS
Protease inhibitors • Metabolic toxicities • Hyperlipidemia/Hypertriglyceridemia-RTV • Hyperbilirubinemia-ATZ and IDV • Nephrolithiasis-IDV (a few case reports with ATZ) • Pyuria and Interstitial nephritis-IDV • Hyperglycemia-IDV and LPV/RTV • Diarrhea-LPV/RTV (cap)& NFV • CAD • Lipodystrophy • Drug drug interactions • Increased bleeding among hemophiliacs • PR interval prolongation-ATZ
Life threatening toxicities • Abacavir hypersensitivity reaction • Lactic Acidosis with NRTI • Nevirapine related hepatotoxicity • Steven Johnson’s syndrome
Fusion inhibitors • Injection site reaction almost universal • Hypersensitivity reaction <1%- do not rechallenge • Increased rate of bacterial pneumonia
A 35 year old female with HIV infection presents to the office. She was diagnosed with PCP and at that time had a CD4 count of 92/µL, viral load-105,000 copies/ml. AZT/3TC/EFV was initiated and 6 months post therapy her CD4 count was 323/µL and her VL was ND. Approximately 1 year ago she started missing appointments and 4 months prior her VL was 878 copies/ml and today her CD4 count is 300/µL and her VL is 5375 copies/ml. She remains asymptomatic. Which of the following is the most appropriate management? • Continue the current regimen • Substitute Nevirapine for Efavirenz • Add Nevirapine to the current regimen • Order an HIV genotype resistance assay • Recommend a drug holiday until she becomes symptomatic.
DHHS guidelines • Monitoring of therapy • Average gains- 50-150 cells/first year and 50- 100 cells/year (assuming viral control) thereafter until a set point is reached • Viral load suppression to below undetectable should be achieved in 16-24 weeks in an ARV naïve patient • A 1 log decline in viral load in 2-8 weeks • Viral suppression in 12-24 weeks
Opportunistic Infections • Fever and Pulmonary infiltrate • CNS manifestations • Ophthalmologic manifestations • Diarrhea
Fever and Pulmonary infiltrate • A 32 year old male presents to the clinic with a 2 week history of non-productive cough, worsening SOB and fever. The patient was recently diagnosed with HIV and his CD4 count is 150 cells/µL. • O/E- HR-100, RR-22, T-100, Pulse ox-85% RA. • RS- examination reveals a few scattered rales and rhonchi.
Differential Diagnosis • PCP- the most commonly diagnosed OI in North America • M.tuberculosis • Community acquired pneumonia • C.neoformans • H.capsulatum • C.immitis • R.equi • Atypical Mycobacteria (M.kansasii) • HSV • CMV • KS • Malignancies
Case • A 40 year female is bought in by her family. Over the past few weeks her family has noticed that she has been forgetful, lethargic and confused. The patient has a CD4 count of 35 and has not been on ART or prophylaxis. • Examination reveals a right sided hemiparesis and VII nerve palsy
Differential Diagnosis By Presenting Symptoms, Exam Findings • Nonfocal • Cryptococcal meningitis • CMV encephalitis • AIDS dementia • Lymphomatous meningitis • Other (TB, fungal) • Focal • Toxoplasmosis • Lymphoma • PML • Cryptococcoma • VZV • Meningovascular • syphilis • Other (TB, fungal)
Is This CNS Toxoplasmosis? • Factors that lessen the likelihood: • On TMP-SMX or other prophylaxis • CD4 count > 100/μl • Negative serologies • Solitary lesion on MRI (multiple and bilateral lesions more c/w toxo) • No contrast enhancement • No MRI improvement on 2-3 weeks of therapy • Uptake on SPECT
Primary AIDS-Related CNS Lymphoma • Mean CD4 = 30/μl • EBV associated • RARE among HIV negative patients about 2% of AIDS patients • Evolution: 2-8 weeks • Survival after diagnosis is usually limited to months • PCR of CSF is usually positive for EBV