Download
1 / 1
70 likes | 490 Views
The Impact of Postpartum Haemorrhage (PPH) on Maternal Morbidity A Mackeen , SY Khong Department of Obstetrics and Gynaecology , University Malaya Medical Centre (UMMC) , Malaysia. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. RESULTS. ABSTRACT. RESULTS. CONCLUSION.

E N D
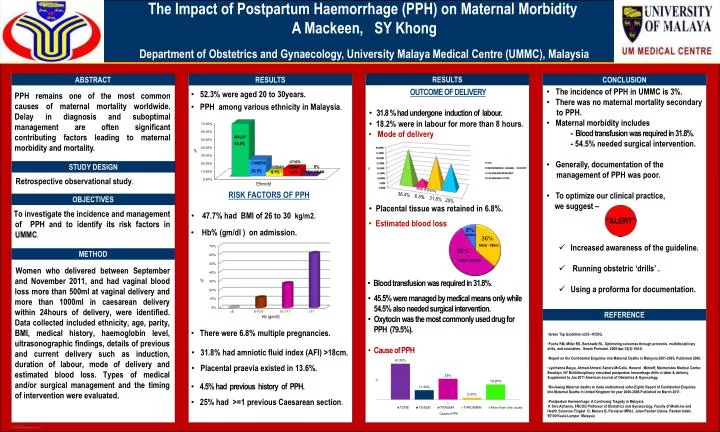
The Impact of Postpartum Haemorrhage (PPH) on Maternal MorbidityA Mackeen, SY Khong Department of Obstetrics and Gynaecology, University Malaya Medical Centre (UMMC), Malaysia OPTIONALLOGO HERE OPTIONALLOGO HERE RESULTS ABSTRACT RESULTS CONCLUSION • The incidence of PPH in UMMC is 3%. • There was no maternal mortality secondary • to PPH. • Maternal morbidity includes • - Blood transfusion was required in 31.8%. • - 54.5% needed surgical intervention. • Generally, documentation of the • management of PPH was poor. • To optimize our clinical practice, • we suggest – • Increased awareness of the guideline. • Running obstetric ‘drills’ . • Using a proforma for documentation. • OUTCOME OF DELIVERY • 31.8 % had undergone induction of labour. • 18.2% were in labour for more than 8 hours. • 52.3% were aged 20 to 30years. • PPH among various ethnicity in Malaysia. PPH remains one of the most common causes of maternal mortality worldwide. Delay in diagnosis and suboptimal management are often significant contributing factors leading to maternal morbidity and mortality. • Mode of delivery • MALAY • 65.9% • % • OTHER- • ASIAN • CHINESE STUDY DESIGN • 0% • INDIAN • % • 20.5% • 9.1% • 4.5% • NON-ASIAN • Retrospective observational study. • Ethnicity • RISK FACTORS OF PPH • 47.7% had BMI of 26 to 30 kg/m2. • Mode of delivery 36.4% 6.8% 31.8% 25% OBJECTIVES • Placental tissue was retained in 6.8%. To investigate the incidence andmanagement of PPH and to identify its risk factors in UMMC. • Estimated blood loss • Hb% (gm/dl ) on admission. • >2000ml • 500ml - 999ml METHOD • 1000ml - 2000ml Women who delivered between September and November 2011, and had vaginal blood loss more than 500ml at vaginal delivery and more than 1000ml in caesarean delivery within 24hours of delivery,were identified. Data collected included ethnicity, age, parity, BMI, medical history, haemoglobin level, ultrasonographic findings, details of previous and current delivery such as induction, duration of labour,mode of delivery and estimated blood loss. Types of medical and/or surgical management and the timing of intervention were evaluated. • Blood transfusion was required in 31.8%. • 45.5% were managed by medical means only while • 54.5% also needed surgical intervention. • Oxytocin was the most commonly used drug for • PPH (79.5%). • Cause of PPH REFERENCE • Hb (gm/dl) • Green Top Guideline no52 –RCOG. • Fuchs KM, Miller RS, Berkowitz RL. Optimizing outcomes through protocols, multidisciplinary drills, and simulation.SeminPerinatol. 2009 Apr;33(2):104-8. • Report on the Confidential Enquiries into Maternal Deaths in Malaysia 2001-2005, Published 2008. • JyothshnaBayya, Ahmed Ahmed, Sandra McCalla, Howard Minkoff, Maimonides Medical Center, Brooklyn, NY Multidisciplinary simulated postpartum hemorrhage drills in labor & delivery. Supplement to Jan 2011 American Journal of Obstetrics & Gynecology. • Reviewing Maternal deaths to make motherhood safer-Eighth Report of Confidential Enquiries into Maternal Deaths In United Kingdom for year 2006-2008.Published on March 2011. • Postpartum Haemorrhage: A Continuing Tragedy in Malaysia • K Siva Achanna, FRCOG Professor of Obstetrics and Gynaecology, Faculty of Medicine and Health Sciences-Tingkat 13, Menara B, Persiaran MPAJ, JalanPandanUtama, Pandan Indah, 55100 Kuala Lumpur, Malaysia • There were 6.8% multiple pregnancies. • 31.8% had amniotic fluid index (AFI) >18cm. • Placental praevia existed in 13.6%. • 4.5% had previous history of PPH. • 25% had >=1 previous Caesarean section. • % • Causes of PPH