Download
1 / 33
330 likes | 341 Views
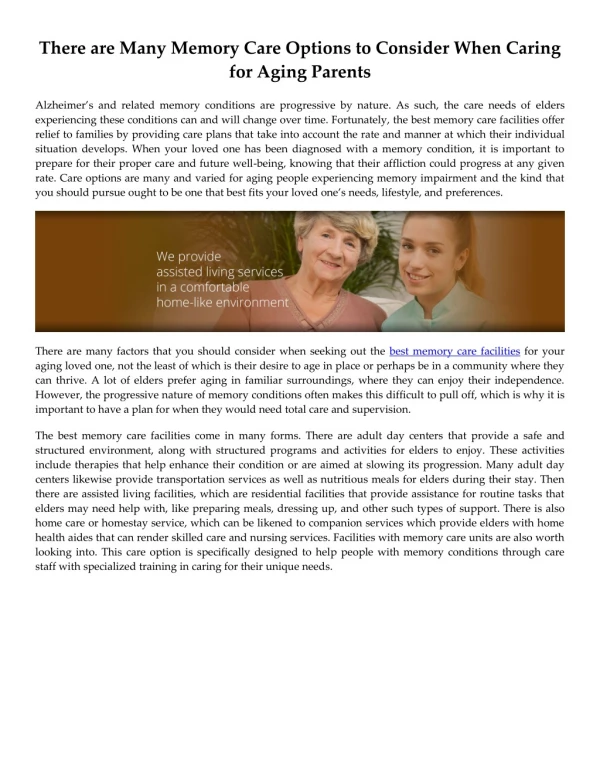
Learn practical strategies for dealing with housing, legal issues, caregiver support, preventive care, and common medical problems in caring for aging parents. Communicate effectively, navigate end-of-life care, and ensure quality support.

E N D
How to Care for Aging ParentsThomas Cornwell, MD How To Care For Aging Parents Thomas Cornwell, MD HomeCare Physicians
Why is this an Issue Now? • 10,000 new Medicare beneficiaries daily
Sandwich Generation • Nearly half of middle-aged adults are either raising a young child or financially supporting a grown child • About one in seven middle-aged adults is providing financial support to both an aging parent and a child Source: http://www.pewsocialtrends.org/2013/01/30/the-sandwich-generation
Talk, Talk, Talk • Issues: • Parenting your parent (Geriatric un-development) • Housing options (now and future) • Financial and legal • Healthcare • Death and funeral (“Honoring ceremony”) • Guiding principles: • Start with areas of agreement • Have entire family on the same page in regards to responsibilities and patient goals • Avoid highly charged and emotional words • Goal is to end all discussions peacefully and to not seek victory
Housing Options • Accessory (in-law) apartments • Shared and congregate housing • Shared apartments • Assisted living • Life care retirement communities • Nursing homes • Live-in caregivers • Guiding principles: • Try to discuss and plan before a crisis occurs • What are the options if/when you or your loved one declines?
Legal Issues • Living will • Durable power of attorney for healthcare and finances • Advanced directives • “Do not resuscitate” form/”POLST” form • Last will and testimony • National Academy of Elder Law Attorneys • Naela.com • 602.881.4005
Caring for the Caregiver • Set limits • Accept and enlist help • The Family and Medical Leave Act allows for 12 weeks of unpaid leave to care for family member • Emotional minefields: Guilt and helplessness • Maintain your physical, emotional and spiritual life
Preventive Care • Yearly flu shot • Pneumonia shot once, or twice five years apart, after age 65 • Tetanus shot every 10 years • Balanced diet • Exercise • Multivitamin • No smoking • Osteoporosis screening
Doctor Visits • Avoid ageism • Bring all medications to visit • Bring list of concerns
Medical Care • Yearly eye and dental exam (Audiologist if there is a hearing problem) • Medical alert system (e.g. Lifeline, Medical Alert) • Medications—the less the better • Ways to save money: • Ask pharmacist if there is a generic equivalent or a larger pill that can be broken in half • Pharmaceutical discount cards or indigent programs
Common Medical Problems • Falls—most common in bathroom • Pressure sore prevention: • Avoid same position for more than two hours • Pressure-reducing surfaces on hospital bed/wheel chairs • No donut cushion • Reduce friction • Signs of depression: • Depressed mood • Anger • Anxiety • Decreased motivation • Anhedonia • Loss of appetite • Trouble sleeping
Dementia • Descriptive diagnosis of abnormal memory loss and cognitive functioning • Greatest problem is short term memory loss is often not realized by patient (and sometimes family) • Agitation can be a major problem • Speak in a slow, calm voice • They are “always” right • Redirect when they are upset—they can only focus on one thing at a time • They use “cues” in their environment to orient themselves, and caregivers can take advantage of this (calendars, leaving messages, etc.) • Consider neuropsychiatric testing for more definitive diagnosis and coping strategies
Hospitalization • Elderly need to have an advocate • Discharge planning begins day one of hospitalization • Is going home an option? • Will rehabilitation be necessary/helpful?
Medicare/Medicaid Intermittent Home Health • Must be homebound • Must have a need for a skilled nurse, physical therapist or speech therapist • If above criteria are met, they can also get an occupational therapist, social worker and aide if necessary • Medicare and Medicaid do not pay for home health when only custodial care is needed
Quality Vs. Crisis End-of-Life Care “The death of a loved one will always be sorrowful, but it does not need to be a crisis. It tends to be a crisis in our country, because we avoid talking about it and planning for it.” - Dr. Thomas Cornwell
End-of-Life Care • “To whatever extent you are able, acknowledge this dying process and, in doing so, celebrate life.” • Start communicating preferably before he/she is sick • Responses to a terminal diagnosis: • Denial • Anger • Bargaining • Depression • Acceptance • Greatest fear of terminally ill: Suffering and abandonment—not death • Hospice care: • Life expectancy less than six months • Patient does not desire aggressive curative care but does want aggressive comfort care
Communication is Key • Hospice is a two-way evaluation • Hospice evaluates if the patient meets Medicare criteria • Patient/family evaluate if they would benefit from hospice • Hospice is an interdisciplinary home health service for patients whose prognosis is less than six months • Doctors and patients are poor at predicting when end-of-life will occur, which leads to: • 10% of hospice patients dying on day one • Over 50% of patients dying in the first two weeks • A good question to ask is, “Would you be surprised if the patient passed away in the next six months?”
Communication is Key (continued) • Patients/families need to know their options: • DNR (DNAR)/POLST • Hospitalization • Ventilator • Tube feedings • Dialysis • Antibiotics • Preferred site of death
Five Wishes Document • The person I want to make care decisions for me when I can’t • The kind of medical treatment I want or don’t want • How comfortable I want to be • How I want people to treat me • What I want my loved ones to know
Wish 1: The Person I Want to Make Health Care Decisions for Me When I Can’t Make Them for Myself • Picking the right person to be your healthcare agent: • Knows you well • Can make difficult decisions • Will stand up and advocate for you • Lives nearby • Must be at least 18 years old • Should not be your healthcare provider or employee of your healthcare provider • Communication your wishes with your healthcare agent: • What level of medical care is desired and for how long? • What level of psychiatric care is desired? • Release of medical records • Organ donation • Review financial information and insurance forms • Desired location to spend your last days/hours
Completing Five Wishes • Sign and fill in demographic information • Have two witnesses sign • No notarization required in Illinois • Distribute copies and discuss with POAHA, family, medical provider, nursing home, assisted living facility, etc. • Fill in Five Wishes Wallet Card and keep it with you to notify people where to locate the document
DNR (Do Not Attempt Resuscitation)/POLST Form • Only document paramedics can accept to not do CPR • Must be signed by patient, guardian, POA or healthcare surrogate • Must have a witness • Must be signed by a doctor • State of Illinois transitioning to POLST (Physician Orders for Life Sustaining Treatment) form
The “Honoring” Ceremony • The funeral/memorial service is our last chance to honor them, but we usually give ourselves only 3-4 days to prepare • It is never too early to start planning the “honoring” ceremony • When the time comes, you will know you are doing exactly what they wanted, and the time is much less stressful
Quality/Cost of End-of-Life Care • Nationally, only 25% of deaths occur at home, although more than 70% of Americans say that this is where they would prefer to die • The 75% of patients that die in hospitals and nursing homes often receive high-tech interventions and are in pain • 26% of Medicare funds are spend on care in the last year of life; 38% of this is spent in the last 30 days
HomeCare Physicians’ Mission • Improve the quality of life of homebound patients • Improve the quality of life of caregivers • Decrease healthcare costs by enabling patients to remain at home and avoid expensive emergency departments, hospitals and nursing homes
Three Reasons for the Decline of the House Call • Increased office/hospital-based technology • Fear of increased liability • Financial disincentives
Why Home Care Medicine’s Time Has Come • Demographics: The aging of society • Technology allows quality care in the home • Cost savings
5/14/09—2/18/11 (1 year, 9 months) • 44 Emergency Department (ED) visits (average 16 days between visits) • 27 hospitalizations—over half required ICU days (average 25 days between stays) • HCP first visit 3/2/11 (365 days) • One ED visit and one hospitalization (May 2011) • Expected: 25 ED visits and 15 hospitalizations • One year cost savings: $188,000
High-Cost Medicare Beneficiary Spending Source: Congressional Budget Office based on data from the Centers for Medicare and Medicaid Services. Note: Spending reported in 2005 dollars
Costs of Care Before Vs. During HBPC for 2002 * Includes HBPC cost
Potential Savings • Illinois population = 12,869,257 • 12.7% > 65 = 1,634,396 • 3.4% ≥ 3 ADL deficiencies = 55,569 • VA saved $9,132 per HBPC patient • Total yearly savings = $507,460,233
Thank you • Thanks to legislative sponsors Senators Jim Oberweis and Linda Holmes and Representatives Linda Chapa LaVia, Mike Fortner and Kay Hatcher ●Thomas.Cornwell@nm.org ● http://rmg.nm.org/what-we-offer/specialized-care/home-care