Download
1 / 43
440 likes | 597 Views
Shaken Baby Prevention Education for Providers. Goals of the Shaken Baby Prevention Program. Decrease the incidence of Shaken Baby Syndrome (SBS) in the military Grow stronger military families by preventing family violence

E N D
Goals of the Shaken Baby Prevention Program • Decrease the incidence of Shaken Baby Syndrome (SBS) in the military • Grow stronger military families by preventing family violence • Educate and influence new parents as they develop effective parenting skills
What do Healthcare Providers need to know about SBS? • Review the incidence, risk factors, presentation and prognosis of Shaken Baby Syndrome (SBS). • Discuss the role of healthcare staff in educating military families. • Highlight the value in education to decrease the incidence, morbidity and mortality of SBS.
Shaken Baby Prevention Action Plan • Provide one-on-one SBS education to parents of every child born in a MTF including deployed new fathers • Ask every new parent to voluntarily sign a commitment statement acknowledging receipt of SBS information about the dangers and consequences of SBS • Educate and encourage fleet healthcare providers to address prevention of SBS and family violence with sailors and marines
Definition • SBS is defined as a non-accidental traumatic injury resulting from violent shaking of an infant or child.
What is the History of Shaken Baby Syndrome ? • Original description “Whiplash Shaken Baby Syndrome” (Caffey, 1970) • Retinal hemorrhages • Subdural and/or subarachnoid hemorrhage • Little or no evidence of external trauma • May or may not have associated fractures
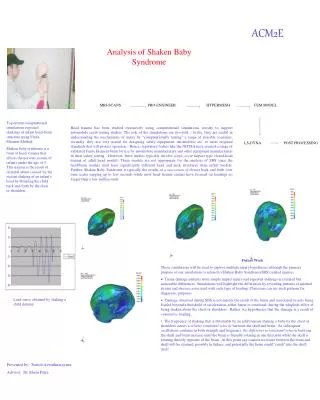
What is the mechanism of injury? • The rapid and repetitive flexion and extension of the neck and head leads to two main types of injury: • Direct trauma to the brain as a result of it striking the skull; • Disruption of bridging vessels that surround the brain, leading to hematoma formation (most common pathologic intracranial finding associated with SBS).
Fast Facts For Discussion • Abusive head trauma is the leading cause of trauma related deaths among children (AAP Policy Statement, July 2001) • 80% of head trauma deaths in infant and children < 2 years were due to child abuse (Bruce and Zimmerman, 1989) • Estimated 3.3 to10 million children witness violence between intimate partners each year (Family Violence Prevention Fund, September 2002) • Concurrence of child abuse and domestic violence 30-60% (Edelson, 1999)
What are the Consequences of Shaking a Baby? • Babies are not able to fully support their heavy heads. As a result, violent and forceful shaking causes a baby's brain to be injured. Too often, this leads to the death of a baby. It also can lead to: • Bleeding around the brain • Blindness • Hearing Loss • Speech or learning disabilities • Chronic seizure disorder • Brain damage
What is the Incidence of Shaken Baby Syndrome in Children under 1 year of Age?(inflicted Traumatic Brain Injury – iTBI) • 29.7/100,000 in NC Keenan et al, 2003 (odds ratio 4.7 for military dependents) • 24.6/100,000 in Scotland Barlow & Minns, 2000 • Over 1400 cases annually in the U.S.
Known Military Cases of SBS • 44 SBS cases in last 18 months as of SEP05 per Armed Forces Center for Child Protection • 30% of cases are USN/USMC families • Likely only the tip of the iceberg • There are no clear reporting mechanisms in DoD • These cases were all preventable!
What is the outcome of SBS? • 1/3 die (mortality 15-38%) • 1/3 severe disability • 1/3 short-term “normal” 1/2 will develop late findings: microcephaly, developmental delay, learning disability, mental retardation, psych/behavior difficulties, seizures, blindness, paralysis
Estimated Cost of Shaken Baby Syndrome* • $60,000 • Initial hospitalization • $100,000 • First year treatment & rehabilitation • $4 -14 Million • Lifetime care of each child victim * University of Pennsylvania Data
What usually triggers the violent shaking event? • Momentary loss of control • Frustration, anger, even rage response by caretaker • Infant crying and fussiness - persistent, inconsolable
Crying Facts for Discussion • Peak age 2-3 months • Unpredictable • Resistant to soothing • Painful facial expression • Long bouts, lasting 30-40 minutes or MORE! • Evening crying • Babies outgrow it!
2/3’s of victims are < 6 months age Roughly equal male/female victim ratio First baby for that family Offenders: biological father Offenders: married to mother Offenders: active duty males 20-25 years old Alone acting as caretaker at time of incident “Crying” as trigger USAF SBS Data Review 2002, USN DoD Data Search 2004 Military Shaken Baby Syndrome Cases
Infant Risk Factors • Frequent crying, inconsolable, “colicky” • Small body size • Large ratio of head to body size • Weak neck muscles • Lack of head control • Prematurity • Special needs • Low birth weight • Poor bonding • Less than 12 months of age • Male
Caregiver Risk Factors • Male (70%) • Single Parent • Low education level • Impulsive or childish behavior • Depression • Mentally challenged • Domestic violence
Environmental and Social Risk Factors • Social isolation • Lack of social support • Low income • Poor prenatal care • Diminished marital satisfaction • Poor family functioning
Clinical Presentation of SBS • Seizures • Apnea/Respiratory Arrest • Loss of consciousness • Vomiting • Lethargy • Irritability
Consequences of SBS • Increased intracranial pressure results from the hemorrhage, cerebral edema, and increased cerebral blood flow from the injury. • Death is usually the result of uncontrolled cerebral edema.
Shaken Baby on Life Support in Pediatric Intensive Care Unit
Analysis of Missed Cases of Abusive Head Trauma,Jenny et al, JAMA 1999;281:621-626 Physicians failed to diagnose abusive head trauma at 1st visit 31.2% of the time (N=173) • Age: younger • Race: more likely to be Caucasian • Family: more likely live with both parents • Severity of Symptoms: more likely be seen for nonspecific vomiting or irritability
Tips for not missing an SBS case • Look for the presence of bruises or abrasions on the faces or heads of children presenting with non-specific symptoms. • Consider head trauma in the differential diagnosis, when evaluating infants and toddlers with non-specific symptoms (such as vomiting, fever, or irritability). • Perform a head-to-toe physical examination, check the fontanelles (soft spots) on the babies heads, measure the head size and be alert for signs of trauma. • Look for signs of previous bleeding or old blood in the spinal fluid when doing a spinal tap • Consult pediatric radiologists to interpret X-rays and head CTs in cases of suspected child abuse.
Reporting Suspected Child Abuse • The Child Abuse Prevention and Treatment Act of 1974 is a federal law that requires mandatory reporting of abuse by designated personnel. • Physicians are required to report in all 50 states whenever abuse is suspected. • Proof is NOT required.
Reporting Guidance • It is good practice to inform families when suspected abuse is being reported. • This helps maintain communication and trust. • If any safety concerns are raised, child protective services, police, or facility security should be present when the family is notified.
State Laws Mandating SBS Parental Education • Florida “Kimberlin West Act” since 2002 • New York since 2001 • Pennsylvania and Maryland have legislation pending
Prevention Education Works • The New York State hospital-based parent education program (Dias Model) targeted parents of all newborn infants. • This education program demonstrated a decrease in the incidence of abusive head trauma injuries by 47% during a 6 year period.
DOSE DATE Caregiver Clients Location Format #1 OB, 3rd ∆ RN, MD Mom or Mom & Dad OB/FP Clinic Screening for risk; New Parent Support Visiting RN referral #2 Birth RN Mom & Dad Hospital Video; one-on-one discussion; SBS brochure; commitment statement #3 2-6 weeks of age Home RN, “Doc”, or senior enlisted educator Mom & Dad Home, Workplace, Medical Clinic Video (if not seen) One-on-one question & answer Group discussion #4 2, 4, 6 MOS WB MD or “Doc” Mom & Dad Medical Clinic Anticipatory guidance to Mom & Dad at well baby visits Schedule of SBS Interventions
The Shaken Baby Prevention Process: Teach & Reach • View Video: 11 minutes • Discussion with healthcare provider* • Voluntary signature on commitment statement • (*Experienced senior enlisted mentors may also deliver this important message to shipmates and new fathers)
Fleet Initiative • Operational HCPs incorporate SBS in new father debriefing sessions while returning to home port • Training Toolkit available on NMO web site: • http://navymedicine.med.navy.mil/womenshealth/ • New fathers educated and given fact sheet • New fathers sign voluntary commitment statement (VCS) • Medical Staff send VCS to Armed Forces Center for Child Protection
Other Efforts to Reach Deployed Fathers • OB prenatal screen to identify deployed parents and families needing support of home visitation RN • Fleet and Family Support: Baby Boot Camp; Couples Communication Classes • Fleet Medical Briefs – Tackle transition back to family life • Chaplain Programs – Marriage & Family Enrichment • Health Promotion & Wellness – Being A Fit Father • Father friendly Well Child Care visits with healthcare provider
Military Families Need to Have a Plan When the Baby Won’t Stop Crying • Stop! Take a time-out, call for help • Call a friend, relative or neighbor for support and advice. • Ask another adult to take care of the infant while you take a break. • Call a crisis hotline (1-800-4-A-CHILD). • Call your health care provider.
References • Keenan HT et al. A Population-Based Study of Inflicted Traumatic Brain Injury in Young Children. JAMA. 2003; 290(5): 621-6 • Herman-Giddens ME. Reducing Collateral Damage on the Home Front: Child Abuse Homicides within Military Families and Communities in North Carolina. September 2004, North Carolina Child Advocacy Institute: www.ncchild.org/maltreatment.htm • USUHS Courage to Care: www.usuhs.mil/psy/courage.html • American Academy of Pediatrics www.aap.org
National Center on Shaken Baby Syndrome 2955 Harrison Blvd Suite 102 Ogden, UT 84403 (801) 627-3399 or 1-888-273-0071 http://www.dontshake.com The Shaken Baby Alliance P.O. Box 150734 Fort Worth, TX 76108 (877) 6-END-SBS http://www.shakenbaby.com US Department of Health and Human Services http://www.hhs.gov American Academy of Pediatrics 141 Northwest Point Blvd Elk Grove Village, IL 60007-1098 (847) 434-4000 http://www.aap.org/ Prevent Child Abuse America 200 S. Michigan Avenue 17th Floor Chicago, IL 60604-2404 (312) 663-3520 http://www.preventchildabuse.org Childhelp USA (Hotline) (800) 4-A-CHILD National Committee To Prevent Child Abuse (Hotline) (800) CHILDREN Resources