Download
1 / 1
10 likes | 140 Views
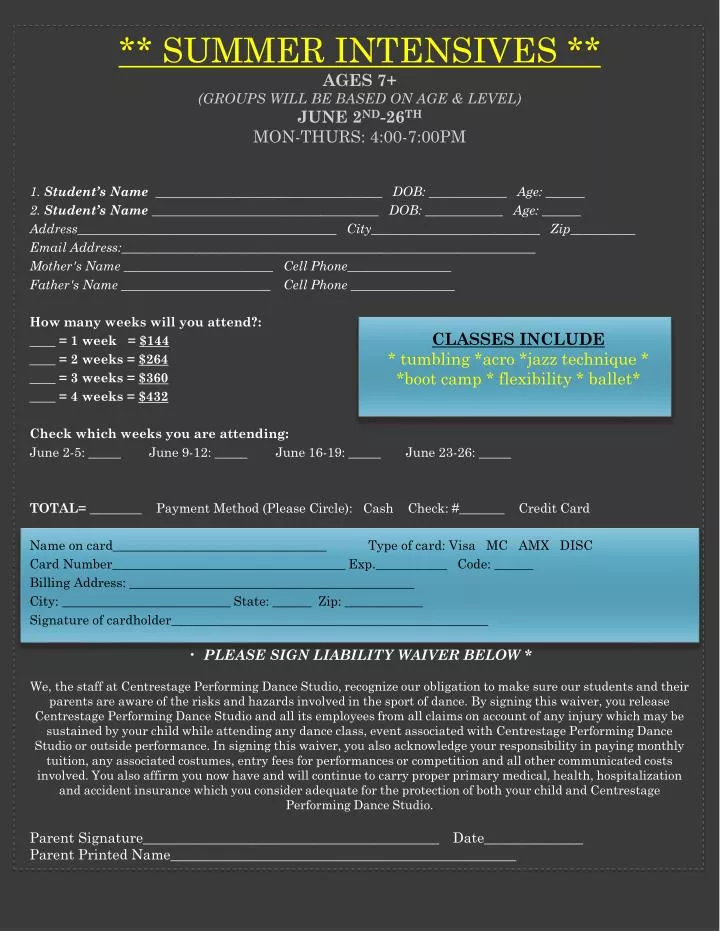
CLASSES INCLUDE * tumbling * acro *jazz technique * * boot camp * flexibility * ballet*. ** Summer Intensives ** AGES 7+ (groups will be based on age & level) June 2 nd -26 th Mon-Thurs: 4:00-7:00pm. PLEASE SIGN LIABILITY WAIVER BELOW *

E N D
CLASSES INCLUDE * tumbling *acro *jazz technique * *boot camp * flexibility * ballet* ** Summer Intensives **AGES 7+ (groups will be based on age & level)June 2nd-26thMon-Thurs: 4:00-7:00pm • PLEASE SIGN LIABILITY WAIVER BELOW * • We, the staff at Centrestage Performing Dance Studio, recognize our obligation to make sure our students and their parents are aware of the risks and hazards involved in the sport of dance. By signing this waiver, you release Centrestage Performing Dance Studio and all its employees from all claims on account of any injury which may be sustained by your child while attending any dance class, event associated with Centrestage Performing Dance Studio or outside performance. In signing this waiver, you also acknowledge your responsibility in paying monthly tuition, any associated costumes, entry fees for performances or competition and all other communicated costs involved. You also affirm you now have and will continue to carry proper primary medical, health, hospitalization and accident insurance which you consider adequate for the protection of both your child and Centrestage Performing Dance Studio. • Parent Signature__________________________________________ Date______________ • Parent Printed Name_________________________________________________ 1. Student’s Name ___________________________________ DOB: ____________ Age: ______ 2. Student’s Name ___________________________________ DOB: ____________ Age: ______ Address________________________________________ City__________________________ Zip__________ Email Address:________________________________________________________________ Mother's Name _______________________ Cell Phone________________ Father's Name _______________________ Cell Phone ________________ How many weeks will you attend?: ____ = 1 week = $144 ____ = 2 weeks = $264 ____ = 3 weeks = $360 ____ = 4 weeks = $432 Check which weeks you are attending: June 2-5: _____ June 9-12: _____ June 16-19: _____ June 23-26: _____ TOTAL= ________ Payment Method (Please Circle): Cash Check: #_______ Credit Card Name on card_________________________________ Type of card: Visa MC AMX DISC Card Number____________________________________ Exp.___________ Code: ______ Billing Address: ____________________________________________ City: __________________________ State: ______ Zip: ____________ Signature of cardholder_________________________________________________