Download
1 / 41
410 likes | 453 Views
Learn how empowering poor people can make services work for them. Explore innovative solutions and accountability frameworks.

E N D
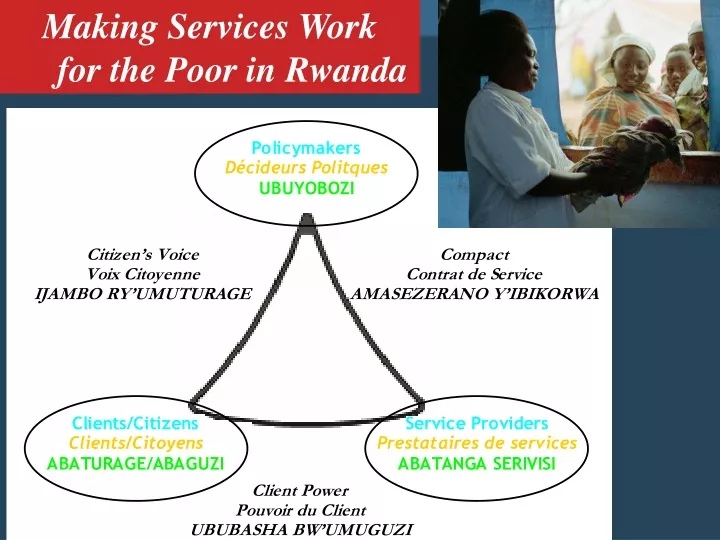
Making Services Work for the Poor in Rwanda
WDR04 Messages • Services are failing poor people. • But they can work. How? • By empowering poor people to • Monitor and discipline service providers • Raise their voice in policymaking • By strengthening incentives for service providers to serve the poor
A framework of relationships of accountability Poor people Providers
In Rwanda • Education:demand side transfers for secondary school tuition for poor children, PTAs • Health: social marketing, drug revolving fund, subsidies to premiums of micro-insurance (mutuelles), participatory health committees • Water: co-payments • Energy: tariff structure • Agriculture: vouchers for extension services?
A framework of relationships of accountability Policymakers Poor people Providers
In Rwanda • Citizen report cards in health, education and administrative services • Community Score cards • Ombudsman office and local conciliators • Civil society review of PRSP monitoring
A framework of relationships of accountability Policymakers Poor people Providers
In Rwanda • Education : Capitation grant to schools • Health: Community Schemes, Performance Based Contracts for health centers • Water: contracts with private operators • Energy: management contract for utilities
598 000 p 200 000 60 000 167 000 p Rwanda : Evolution of expenditures and number of additional people having access to water
Decentralizing • Make services closer to clients ? • Make government closer to citizens ? • Make government closer to services ?
What not to do… technocratic solutions… Of course we have progressed a great deal, first they were coming by bullock-cart, then by jeep and now this!
What is to be done? Tailor service delivery arrangements to service characteristics and country circumstances
Why don’t services work for poor people? Ah, there he is again! How time flies! It’s time for the general election already! By R. K. Laxman
PRONASOL expenditures according to party in municipal government Source: Estevez, Magaloni and Diaz-Cayeros 2002
Clientelistic politics • Can be measured: benefit incidence • Dynamic • Political process complex: both pro-poor and clientelistic streams • Working at the margin: opportunities
Making Services Work for Poor People Expenditure incidence Health Education Source: Filmer 2003b
Homogeneous • 1. “Externality” • Public Good: eg air and water quality, • Externalities: e.g communicable diseases, curriculum, roads, water access • Network externalities: ef electricity grid
Homogeneous 2. Common needs eg • Administrative requirements • Antenatal care/ deliveries/ immunization • School exams/ requirements
Homogeneous 3. Common destiny eg • Policies • Legal framework • Standards
Decentralization and the service delivery framework Center Devolution Sub-national government Policymaker Politicians Politicians Policymaker Voice Delegation Compact Deconcentration Citizens/clients Providers Poor Non Poor Organizations Frontline Client’s power
Decentralization National policymakers Local policymakers Poor people Providers
Easy of difficult to monitor • Three types of monitors: • clients • Policymakers: • Self Regulation of providers
Making Services Work for Poor People The public private mix varies between countries, interventions and income groups
Who can monitor what • Clients can monitor services that are transaction intensive, discretionary and with little asymmetry of information • Eg: use of soap. Handwashing, bed nets, condoms, presence of teachers, presence of nurses, cleanliness of services, quanity and taste of water etc
Who can monitor what • Policymakers can monitor services that are standards and non transaction intensive even with high assymetry of information • E.g: water access, learning of kids, diseases surveillance, quanity and quality of standards services (immunization, antenatal care)
Who can monitor what • Self regulation need to develop when services are both transaction intensive, discretionnary and with high assymetry of information • -eg clinical care: only doctors can monitor doctors, engineers engineering
Which level of government should monitor what • Policymakers can monitor services that are standards and non transaction intensive even with high assymetry of information E.g: water access, learning of kids, diseases surveillance, quantity and quality of standards services (immunization, antenatal care)
Which level of government should monitor what • Consequently adequate level of government responsibility would depend on • 1. capacity to monitor standard services, with a minimum of assymetry of information • 2 capacity to support clients and Citizens in exerting monitoring of discretionary , transaction intensive services • 3 capacity to support self regulation
Making Services Work for Poor People Eight sizes fit all?
Proposed earmarked transfers to manage transition phase(under construction)
Making Services Work for the Poor in Rwanda