Download
1 / 59
780 likes | 1.59k Views
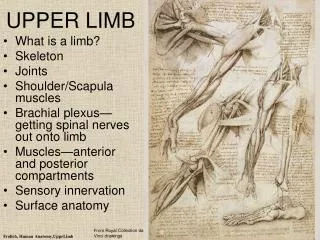
Spasticity and the Botulinum Toxin for the Upper Limb after Stroke (BoTULS) trial. Helen Rodgers Professor of Stroke Care. Spasticity. Upper limb spasticity is a significant problem post stroke. www.wemove.com. Spasticity. But what is spasticity….?

E N D
Spasticity and the Botulinum Toxin for the Upper Limb after Stroke (BoTULS) trial Helen Rodgers Professor of Stroke Care
Spasticity Upper limb spasticity is a significant problem post stroke. www.wemove.com
Spasticity • But what is spasticity….? • Narrow definition: “velocity dependent increase in stretch reflexes” • Wider definition including: • Spasticity as above • Spastic dystonia • Co-contraction • Hyperreflexia/clonus • Spasms • Associated reactions “disordered sensorimotor control, resulting from an upper motor neurone lesion, presenting as intermittent or sustained involuntary activation of muscles” What we recognise clinically
Problems caused by spasticity • Deformity • Pain • Spasms • ‘Passive’ functional limitations (e.g. hand hygiene, dressing a sleeve) • ‘Active’ functional limitations (e.g reaching and grasping)
Treatment of spasticity • Removal of exacerbating factors eg pain • Oral medication eg baclofen • Intrathecal medication (baclofen, phenol) • Phenol nerve blocks • Physical therapy • Botulinum toxin
Botulinum toxin • Protein produced bybacteria Clostridium botulinum • Causes botulism…. • But used therapeutically since 1970’s • Temporarily blocks neuromuscular transmission • Injection weakens muscles • Developed as a treatment for conditions with “overactive muscles” • Squints, dystonias, spasticity • Cosmetic uses: wrinkles
5 2 3 1 4 Botulinum toxin mechanism of action De Paiva A et al, Functional repair of motor endplates after botulinum neurotoxin type A poisoning, Proc Natl Acad Sci USA, 16;96(6):3200-5, 1999
Botulinum toxin for upper limb spasticity post stroke • First used 1989 in observational study - encouraging results • Since then,15 published RCTs (prior to BoTULS) • RCTs of varying methodological quality and size • Unclear randomisation processes • Unclear blinding processes • Unclear if groups differed only in respect to botulinum toxin injections • Unclear if intention to treat analyses carried out • Often no power calculations • Smallest n = 15, largest n = 126 • Plus, variable inclusion criteria, botulinum toxin injection patterns and dosage, outcome measures, follow up times.
Measurement in rehabilitation research • Need to measure functional limitation (and quality of life) as well as impairment (e.g. Spasticity) 1. Measurement of spasticity – “overactive muscles” Traditionally by Modified Ashworth Scale – but measures biomechanical changes as well as spasticity. And, this scale only validated at elbow
Measurement in rehabilitation research 2. Measurement of functional limitation i. Global ADL scales – but lack sensitivity to focal changes Barthel Index
Measurement in rehabilitation research 2. Measurement of functional limitation ii. “Laboratory” like scales – but lack information about “real world” limitation Action Research Arm Test (ARAT) iii. Scales believed to capture “real world” limitation
Botulinum toxin for upper limb spasticity post stroke: results of previous RCTs • All show spasticity (muscle tone on Modified Ashworth Scale…) decreases after botulinum toxin injection
Botulinum toxin for upper limb spasticity post stroke: results of previous RCTs Functional limitation assessed in different ways: i. 4 trials analysed specific basic functional tasks and all showed improvement – “passive function” • opening hand to clean palm • opening hand to cut fingernails • placing arm down a sleeve ii. 6 trials used a scale to report physician and/or patient “global assessment of benefit” and all showed improvement iii. a variety of tools to assess “active function” and global ADL were used but inconsistent results seen – only 1 trial showed improvement
Botulinum toxin for upper limb spasticity post stroke: results of previous RCTs • No improvements in quality of life • Only 2 trials have evaluated repeated botulinum toxin injections showing spasticity decreases • No trial has standardised “other rehabilitation treatments”
Botulinum toxin for upper limb spasticity post stroke: results of previous RCTs • Only strong evidence from previous trials is that botulinum toxin can produce short term decrease in spasticity
BoTULS Botulinum Toxin for the Upper Limb after Stroke
Primary objective To compare the upper limb (UL) function of participants with spasticity due to stroke who receive: • botulinum toxin injection(s) plus an UL therapy programme (intervention group) • UL therapy programme alone (control group) One month after study entry.
Primary outcome measure: Action Research Arm Test Grasp Grip Pinch Gross movements
Secondary objectives • To evaluate impairment (1, 3, 12 months): 2. Grip strength 1. Muscle tone (spasticity) 3. Arm strength: Motricity Index
Secondary objectives 2. Dexterity: Nine hole peg test 4. Barthel ADL Index • To evaluate functional limitation (1, 3, 12): 3. Basic arm activities
Secondary objectives • To evaluate quality of life/participation restriction (1, 3, 12 months): • Euroqol EQ-5D • Stroke Impact Scale • Oxford Handicap Scale • Pain
Methods Multicentre RCT (ran July 05-June 08) • North Tyneside • Wansbeck • Hexham • Newcastle • Sunderland • Gateshead • South Tyneside • Durham • Carlisle • Bishop Auckland • Hartlepool/North Tees
Study flowchart Target population Adults with upper limb spasticity and reduced upper limb function due to stroke > 1 month previously Screeningassessment Baselineassessment CENTRAL RANDOMISATION Website
Study flowchart INTERVENTION Botulinum toxin + 4 week upper limb therapy programme (one hour twice per week provided by study therapist) CONTROL 4 week upper limb therapy programme (one hour twice per week provided by study therapist) 1 month Blinded assessment: outcome measures 3 month Blinded assessment: outcome measures Clinical assessment by study therapist. If required: I : further botulinum toxin and UL therapy. C: further UL therapy 6 month and 9 month Clinical assessment by study therapist. If required: I : further botulinum toxin and UL therapy. C: further UL therapy 12 month Blinded assessment: outcome measures Clinical assessment by study therapist. If further spasticity treatment required, refer to local services or regional spasticity clinic
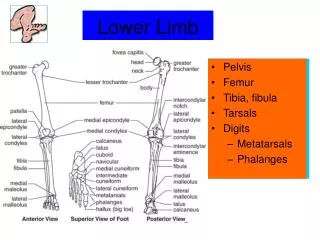
Trial treatments: botulinum toxin • Injected according to spasticity pattern • Commonly chosen muscles: • Hand – FDS, FDP, FPL • Wrist – FCR, FCU • Elbow – biceps, brachioradialis • Shoulder – pec major
Trial treatments: therapy • Menu 1: ARAT 0-3. Stretching, passive and active assisted upper limb movement, hygiene and positioning • Menu 2: ARAT 4-56. Stretching, intensive task orientated practice • 1 hour, 2x/week for 4 weeks
Trial pre-planned statistical analysis • Primary outcome – ARAT • Number of “successful” treatments in each group (control/intervention - ITT) compared (Fisher exact test) • Success • ARAT 0-3 = improve by 3 • ARAT 4-56 = improve by 6 • ARAT > 51 = final score 57 • Power calculation performed on this binary outcome. 332 patients needed to give 80% power to detect a 15% difference in successful treatments between the groups (two tailed, 5%) • Secondary outcomes: binary data, fisher exact/chi square. Remaining data non parametric stats
Trial co-ordination • Research therapist in each site recruited patients and delivered therapy • Patients travelled to either Newcastle or Carlisle to receive botulinum injections • Research therapists performed outcome measures for patients in an adjacent site (blinded) • Central office in Newcastle co-ordinating activity • Randomisation via web • Organise injections • Co-ordinate outcome assessment cover • Handle data • Deliver training • Deal with research governance • Generate reports
Investigational Medicinal Product
Staff • Recruitment and training of staff
Staff • Agenda for Change • Training - Therapy programme - Research methods - Protocol adherence - Research governance
Governance • Local R&D approvals • Acute Trusts and PCT’s • Honorary Contracts • CRB • Sponsorship • Caldicott • Site files • MHRA inspection
Components of success Research skills
But equally important…. …..The Team
Randomised n=333 Intervention n=170 Control n=163 3 Withdrawn 4 Withdrawn 1 Died n=158 n=167 1 Month assessments completed n=155 3 not done 1 Month assessments completed n=167 1 Withdrawn 2 Withdrawn 1 Died 1 Died n=165 n=155 2 not done 3 Month assessments completed n=163 3 Month assessments completed n=151 4 not done 208-7 (withdrawn/died) = 201 patients eligible for 12 month outcome – patients recruited after 1/7/2007 followed for only 3 months 0 Withdrawn 2 Withdrawn 2 Died 4 Died n=99 n=94 2 not done 12 Month assessments completed n=97 12 Month assessments completed n=92 2 not done CONSORT flowchart
Reminder: primary analysis • Primary outcome – ARAT at 1 month • Number of “successful” treatments in each group (control/intervention) compared (Fisher exact test) • Success • ARAT 0-3 = improve by 3 • ARAT 4-51 = improve by 6 • ARAT >51 = final score 57
Results: Primary outcome ► No significant difference between the groups
ARAT Change in score from baseline to 1 month worse better
Results: Secondary outcomes, impairment Muscle tone (spasticity)
Results: Secondary outcomes, impairment Upper limb strength Grip strength: no significant differences