Download
1 / 41
510 likes | 1.27k Views
CALGB 9343 Comparison of Lumpectomy Plus Tamoxifen With and Without Irradiation in Women 70 or Older with Clinical Stage I, ER+ Breast Carcinoma. Kevin S. Hughes, Lauren A. Schnaper, Constance Cirrincione, Donald Berry, Beryl McCormick, Hyman B. Muss, Clifford Hudis, Eric Winer, Barbara L. Smith

E N D
CALGB 9343Comparison of Lumpectomy Plus Tamoxifen With and Without Irradiation in Women 70 or Older with Clinical Stage I, ER+ Breast Carcinoma Kevin S. Hughes, Lauren A. Schnaper, Constance Cirrincione, Donald Berry, Beryl McCormick, Hyman B. Muss, Clifford Hudis, Eric Winer, Barbara L. Smith Cancer and Leukemia Group B Radiation Therapy Oncology Group Eastern Cooperative Oncology Group
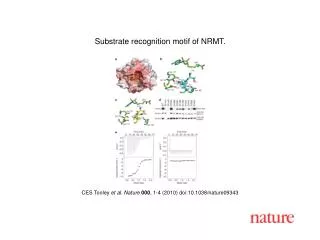
RANDOMIZE CALGB 9343 ELIGIBILITYAge ³ 70 Clinically Node Negative Lumpectomy,Negative MarginTumor size£ 2 cm ER Positive orIndeterminate Radiation Tamoxifen Tamoxifen
Objections to this study • Patients randomized to receive no radiation would be inappropriately under-treated • Patients randomized to receive radiation therapy would be inappropriately over-treated
CALGB 9343 • Opened July 15, 1994 • Closed February 26, 1999 647 patients • Eligible 631 • Ineligible 5 • Canceled/Never treated 11 Median follow-up 12 years
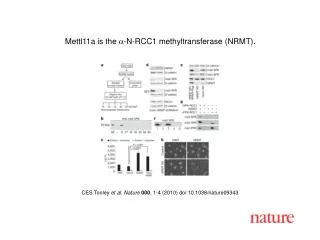
Patient characteristics RT+Tam Tam Total treated 317 319 Age >75 176 (56%) 172 (54%) ER Positive 308 (97%) 310 (97%) Size < 2cm 295 (93%) 296 (93%) No Ax dissection 200 (63%) 203 (64%)
No RT • IBTR 6 • 4 • RT • Mastectomy • 10 • IBTR • 27 • 17 • Lumpectomy
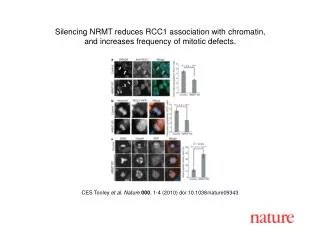
Benefits of RT are small 21 women N (% at 10 yeas) N (% at 10 years)
CONCLUSION: In older women, the benefits of radiation after lumpectomy are small 21 women • Breast recurrence ~7% • Radiate 319 women to avoid 21 in breast recurrences • Ultimate breast preservation NS • Second primary cancer NS • Distant metastases NS • Death breast cancer NS • Death from any cause NS
CONCLUSION: In older women, the benefits of radiation after lumpectomy are small 21 women • Breast recurrence ~7% • Radiate 319 women to avoid 21 in breast recurrences • Ultimate breast preservation NS • Second primary cancer NS • Distant metastases NS • Death breast cancer NS • Death from any cause NS Study is mature: 12 years Median, Half of patients dead With modern margins and AI’s, RT will likely have even less benefit
CONCLUSION: In older women, the benefits of radiation after lumpectomy are small 21 women • Breast recurrence ~7% • Radiate 319 women to avoid 21 in breast recurrences • Ultimate breast preservation NS • Second primary cancer NS • Distant metastases NS • Death breast cancer NS • Death from any cause NS Omitting Radiation in women 70 and above with Clinical Stage I breast cancer is a reasonable alternative for our patients
CALGB 9343 enrolled 647 patients. Eleven patients never began protocol therapy; findings are based upon the 636 patients who began protocol treatment. As of May 2010, the median follow-up for treated patients was 12 years with a maximum of 16 years. Three hundred nine (309) patients are alive and in active follow-up. Two hundred thirty-nine (239, 77%) of them have survived at least 10 years from enrollment. Only four patients (<1%) have been lost to follow-up, and only 10 patients (1.5%) withdrew consent to be followed. Table 1. Patient enrollment Tam + RTTamTotalTotal enrolled323 (100%)324 (100%)647 (100%)Never began Rx6 (2%)5 (2%)11 (2%)Treated317 (98%)319 (98%)636 (98%) Data as of May 2010 Median follow-up = 12 years (range = 1, 16) Table 2. First event The table below describes the first recurrence: local, distant or local and distant synchronously. Because the entries are for first recurrence, a patient may only be counted once. StatusArmTotalTam + RTTamTreated317 (100%)319 (100%)636 (100%)Total recurrences234164Type of recurrencea. Local only42832 In breast only ( 4) (22) (26) Axillary only ( 0) ( 5) ( 5) In-breast + axillary ( 0) ( 1) ( 1)b. Distant only171128c. Local + distant *224 * All local recurrences were IBTR only. Table 3. 10-year incidence of each study endpoint by treatment arm This table considers the occurrence of each event at any time in follow-up. It is therefore unlike Table 2, which is restricted to site of first recurrence only. A patient may have an event for each of the five endpoints. ArmEndpointFree from local recurrenceWithout subsequentmastectomyFree from distant metsOSBC-specific survivalTam + RT98%(96-99%)98%(96-99%)95%(92-97%)67% (61-72%)97%(94-99%)Tam90%(85-93%)96%(93-98%)95%(91-97%)67%(61-72%)98%(95-99%) Table 4. Comparison by treatment arm of entire distribution of each endpoint EndpointTime to local recurrenceTime to subsequent mastectomyTime to distant metsOSBC-specific survivalP-value from logrank test0.00010.180.460.800.41 Table 5. Second primaries SiteArmTotalTam+RTTamBreast Invasive9918 DCIS213 Lymph nodes101Blood AML112 CLL011 MDS011Lymphoma Lymphoma325 NHL112GI Abdomen011 Bowel101 Colon448 Epiglottis101 Peritoneum011 Rectum101 GI, NOS101GU Bladder101 Endometrium314Hepatic Liver022 Pancreas011 Spleen101Lung4711Melanoma202 Two patients had two new primaries.
Can we? Should we? Patient factors are dependent on physiologic age Tumor factors are dependent on chronologic age
Concerns regarding this study Patients randomized to receive no radiation would be inappropriately under-treated
Concerns regarding this study Patients randomized to receive no radiation would be inappropriately under-treated Patients randomized to receive radiation therapy would be inappropriately over-treated
Time to IBTR 20 women
Concerns regarding this study • Patients randomized to receive no radiation would be inappropriately under-treated • Patients randomized to receive radiation therapy would be inappropriately over-treated