Download
1 / 24
240 likes | 272 Views
TRACHEOSTOMY (a life saving procedure). Dr. Abdussalam M jahan ENT depart, Misurata university, faculty of medicine. Introduction.

E N D
TRACHEOSTOMY(a life saving procedure) Dr. Abdussalam M jahan ENT depart, Misurata university, faculty of medicine
Introduction • Tracheostomy:is a surgical opening in the anterior aspect of the neck leading directly to the trachea. It is maintained open with tube called a Tracheostomy tube.
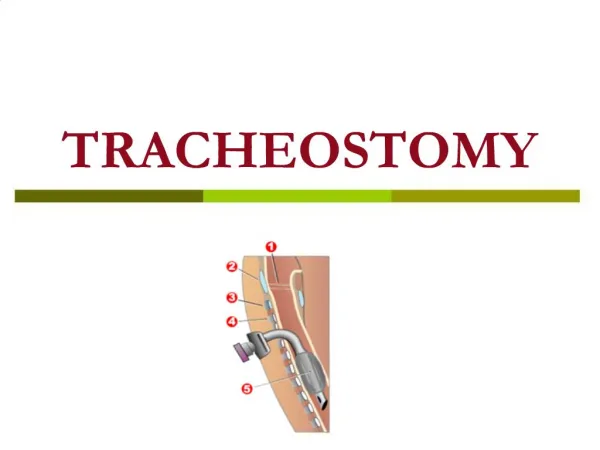
Relevant Surgical Anatomy 1 - Vocal cords 2 – Thyroid cartilage 3 - Cricoid cartilage 4 - Tracheal cartilages 5 - Balloon cuff
Indications: 1-upper airway obstruction, as mass or trauma, where intubation may be impossible. 2- Assist respiration over prolonged periods. 3-prolonged intubation with endotracheal tube: (more than 7-10 days) to reduce the possibility of subglottic stenosis.
4- assist cleaning of lower respiratory tract secretions 5-Facial fracturesthat may lead to upper airway obstruction (eg, comminuted fractures of the midface and mandible) 6-Major operations on the head and neck.
7- Reduce aspiration • 8-Severe obstructive sleep apnea. (if other options failed).
Contraindications • No absolute contraindications exist to tracheostomy • RELATIVE • Laryngeal carcinoma it may lead to increased incidence of stomal recurrence (adiffuse infiltrate of neoplastic tissue at the junction of the amputated trachea and skin )
Types of Tracheostomy Tubes Metal TT
Procedure • Transverse Incision • Incision 1 cm below the cricoid or halfway between the cricoid and the sternal notch.
Procedure cont’d • Blunt dissection of subcut tissue • Transversely retracted as shown
Procedure cont’d • Strap muscles are divided longitudinally at midline
Procedure cont’d • Thyroid ismuth is divided at midline by 2 hemostatic forcepses and cut edge secured by 2/0 vicryl
Procedure cont’d • After exposing of trachea, inverted U opening is made in trachea below 2nd ring
Procedure cont’d • By the Negus forceps the trachea dilated and tracheostomy tube inserted in the inverted U incision.
Procedure cont’d • Fixation of the tube.
Post-Op Management • Repeat X-Ray soft tissue neck • Strong Analgesia • Antibiotics • IV fluid until able to tolerate orally
Complications of Tracheostomy • Complications 5-40% • Mortality <2% • Complications are more frequent in emergency situations, severely ill patients
Immediate complications: • Apnea due to blood clot obstructing the tube, wrong insertion or displacement of the tube. • Bleeding. • Pneumothorax or pneumomediastinum: These can result from direct injury to the pleura or the cupola of the lung (especially in children). • Injury to adjacent structures: paratracheal structures vulnerable to injury are RLN, the great vessels, and the esophagus.
Early complications: • Early bleeding: This is usually the result of increased blood pressure as the patient recovery from anesthesia and begins to cough. Although this may necessitate a return to the operating room, bleeding may be controlled with local packing, cautery, control blood pressure. • Plugging with mucus.
Tracheitis: present in all patients with fresh tracheostomies. humidification, minimization of the fraction of inspired oxygen (FIO2) (because high oxygen levels exacerbate drying), and irrigation are essential. • Cellulitis. • Displacement of the tube.
Subcutaneous emphysema: This results from a tight closure of tissue around the tube, tight packing material around the tube, or false passage of the tube into pretracheal tissues. • Atelectasis: An overly long tube can mimic a unilateral mainstem intubation, causing atelectasis or collapse of the opposite lung.
Late complications: • Bleeding: Bleeding more than 48 hours after the procedure is most commonly (50%) caused by tracheo-innominate erosion (fistula). • Stenosis (subglottic stenosis) • Tracheoesophageal fistula: usually caused by friction between a posteriorly displaced tracheostomy tube or overinflated cuff and a rigid nasogastric tube. It manifests as aspiration and subsequent chemical pneumonia.
Tracheo-cutaneous fistula. • Scarring: Both vertical and horizontal incisions heal with small but visible scars. Clinico-Pathology Seminar: Dept. of ORL, UITH.