Download
1 / 81
820 likes | 1.18k Views
PCOS, dyslipidemia and CVD Nelly Pitteloud, MD Reproductive Endocrine Unit Massachusetts General Hospital COI: Repros Consultant. Objectives. PCOS Definition Pathophysiology Metabolic features. 22 yo woman with oligomenorrhea. 22 yo with 9 months oligoamenorrhea

E N D
PCOS, dyslipidemia and CVDNelly Pitteloud, MD Reproductive Endocrine UnitMassachusettsGeneral HospitalCOI: Repros Consultant
Objectives • PCOS • Definition • Pathophysiology • Metabolic features
22 yo woman with oligomenorrhea • 22 yo with 9 months oligoamenorrhea • Menarche age 11 yrs, cycles approx 45 days • Slightly overweight since elementary school • Acne with menses • Waxes upper lip, chin weekly for one year • Family history of type 2 diabetes
Examination • Weight 178, height 5’5”, BMI 29 kg/m2 • Terminal hair on face • Acanthosis nigricans • Work-up: Neg hCG, FSH 5.2 IU/L, Prl 10 ng/ml, TSH 2.0 uU/ml, T 90 ng/dL Diagnosis? Further work-up?
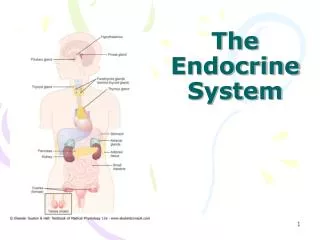
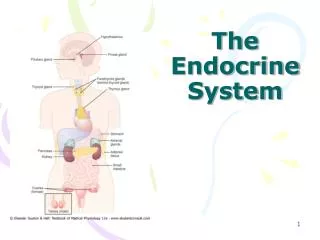
Hypothalamic-Pituitary-Gonadal Axis Hypothalamus GnRH Pituitary LH E2 FSH Ovary
POLYCYSTIC OVARIAN SYNDROMEDefinition 1990 NIH Workshop • CHRONIC OLIGO/ANOVULATION • HYPERANDROGENISM in the absence of other known causes of androgen excess (tumor, CAH, hyperprolactinemia)
POLYCYSTIC OVARIAN SYNDROME2003 Rotterdam Workshop • 2 of 3: • CHRONIC OLIGO/ANOVULATION • HYPERANDROGENISM • POLYCYSTIC OVARIAN MORPHOLOGY in the absence of other known causes of androgen excess
Polycystic Ovarian Syndrome • Affects 6-10% of women of childbearing age (3.2 to 5.4 million women in the U.S.) • Chronic anovulation and hyperandrogenism • Most common cause of female infertility (approximately 50-60%) • Anovulation • Early miscarriage • Most common endocrinopathy in young women • Insulin resistance is a prominent feature
Normal ovary • Few follicles • Random distribution • No increased stroma • Polycystic ovary (PCO) • Ovarian vol >10 ml or • >12 small follicles (2-8 mm) • Peripheral distribution • Increased stromal vol • (Jonard et al, 2003)
Proportion of Anovulatory PCOS Subjects 0 20 40 60 80 100%
POLYCYSTIC OVARY SYNDROME: Clinical concerns • Menstrual cycle irregularity/Chronic unopposed estrogen exposure • Hyperandrogenic symptoms (hirsutism, acne, alopecia) • Anovulatory infertility (but risk of intermittent ovulation) • Metabolic risks
Neuro- endocrine Androgens Insulin Pathophysiology of PCOS Menstrual Irregularity + Hyperandrogenism
Pathophysiology of PCOS Hyperandrogenism ovary 1o or 2o morphology adrenal
PCOS PCOS Normal Normal Taylor et al, 1994
Pathophysiology of PCOS Neuroendocrine abnormalities 1o or 2o? LH FSH Hypothalamus Pituitary
100 LH IU/L 50 PCOS 25 FSH IU/L 20 10 Yen et al, 1970 Gonadotropin Abnormalities in PCOS Normalized transiently after ovulatory cycle or progestin
Pathophysiology of PCOS Hyperinsulinemia insulin signaling SHBG
Insulin Resistance and PCOS • Insulin resistance is a very common feature of women with PCOS (60-75%) • Insulin resistance occurs in both obese and non-obese women with PCOS • Anomalies in insulin Receptor mediated transduction • Obesity has a synergystic effect on glucose metabolism and IR Palomba S, Endocrine Review, 2009
WHO 2006 Criteria to define hyperglycemia 2-h glucose/OGTT NGT <140 mg/dl (7.8 mmol/liter) IGT >140 mg/dl (7.8 mmol/liter) and < 200 mg/dl (11.1 mmol/L) DM = or > 200 mg (11.1 mmol/liter Fasting glucose Normal FG <110 mg/dl (6.1 mmol/liter) IGT 110 mg/dl (6.1 mmol/liter) to 125 mg/dl (6.9 mmol/L) Diabetes = or > 126 mg/dl (7.0 mmol/liter)
* * * * * * 200 LEAN 200 * PCOS * 150 PCOS 150 100 NL 100 50 NL 0 50 0 20 40 60 80 100 120 0 200 0 20 40 60 80 100 120 * 200 * * * PCOS PCOS 150 150 100 NL NL 100 50 50 0 120 0 20 40 60 80 100 0 0 20 40 60 80 100 120 Insulin and Glucose Responses in PCOS OBESE INSULIN GLUCOSE MINUTES Dunaif A et al, 1987
IR is present in both lean and obese PCOS compared to their BMI and age matched counterpart Insulin Sensitivity Nl Lean Nl Obese PCOS Lean PCOS Obese Dunaif A et al, 1987
PCOS and Obesity • 60% of US women with PCOS are obese • Distribution of fat: visceral adiposity (Android pattern) • Known to be metabolically active • Highly associated with hyperinsulinemia • Central obesity correlates with CV risk. • 70% of lean PCOS women have an android pattern of fat distribution. • Is obesity an intrinsic clinical sign of PCOS or promoting environmental factor? • Nelson SM, 2007
Prevalence of Glucose intolerance and Diabetes in PCOS
Prevalence of IGT (by OGTT ) in 254 womenwith PCOS 14-44 yr old 61,3% 31.1% 7.5% NGT IGT Type II DM Legro et al, JCEM, 1999
Conversion rate to IGT and type II DM • Controlled Study • Baseline OGTT • 71 PCOS and 23 normal • F/U 2-3 yr • PCOS: • 37% IGT and 10% DM2 at baseline • 16% conversion/year from NGT to IGT • 2% conversion/year from IGT to DM2 • The conversion from IGT to frank diabetes is substantiallyenhanced in women with PCOS • Legro et al, JCEM, 2005
Development of Gestational DM • Meta-analysis • 720 women with PCOS and 4505 controls • RR 2.94 (CI 1.70-5.08) of developing GDM than controlwomen • Besides converting to IGT or type 2 DM, women with PCOS arealso at high risk for developing gestational DM • Boomsma et al, Hum Reprod Update, 2006
PCOS and Type II diabetes • Nurses’ Health Study II (NHSII): 101.073 women • Women followed for 8 years • Conversion rate to DMII was 2-fold higher in oligo- • menorrheic women, independent of weight • By age 30, 30-50% of obese PCOS developed IGT or DM • 3-7x increase as compared to the general population • Legro et al, JCEM, 1999
Mechanisms of Predisposition to the development Type II DM in PCOS • Women with PCOS are insulin resistant independent of obesity • Defects in insulinreceptor or post-receptor signal transduction • Alteredadipocyte lipolysis • Decrease GLUT-4 expression in the adipocytes • Many PCOS women exhibit β-Cell dysfunction • Ek I et al JCEM 1997 • Ek I et al, Diabetes 2002 • Kelsey ES, JCEM 2007
Metabolic Syndrome NCEP 2001 ATP III > 3 of the following for women: Triglycerides >150 mg/dL HDL Cholesterol (F) < 50 mg/dL Blood Pressure >130/85 mm/Hg Waist > 88 cm Glucose (fasting) > 100 mg/dL
Prevalence of Metabolic syndrome in PCOS • 33.4% of obese PCOS • (Ehrmann et al, 2006) • 24% of PCOS (BMI • = 31 kg/m2) • (Welt et al, 2007) • 37% of adolescent • girls • (Coviello et al 2006) Apridonidze T eta al JCEM 2005
Prevalence of Metabolic syndrome in PCOS compared to NHANES women Age Group BMI (kg/m2) <25 25–30 >30 20–29 yr (n = 29) PCOS (%) 17 58 45 U.S. females (%) 0.8 8.3 27 30–39 yr (n = 49) PCOS (%) 23 40 62 U.S. females (%) 1 14 43 Apridonidze T eta al JCEM 2005
CV Risk Factor in PCOS • Surrogate endpoints suggest increased CV risk: • Hypertension, Obesity, WHI, Insulin resistanc, HDL • TG , Chronic inflammation, C-reactive protein & PAI-1 • Likely due to both: • Hyperandrogenism • Impaired insulin sensitivity
Distribution of CHD risk factors in premenopausal women PCOS vs. control PCOS (n=36) NL (n=71) Pvalue Variable • Age (yr) 38.5 39.0 0.40 • BMI (kg/m2) 31.4 31.2 0.26 • Waist (cm) 94.75 94.5 0.14 • Ferriman-Gallwey 16.0 4.0 0.0001 • Systolic BP (mm Hg) 116 116 0.73 • Diastolic BP (mm Hg) 74.8 71.5 0.03 • Smoking status 8.3% 11.4% • Fasting insulin (µIU/ml) 7.65 6.3 0.11 • Fasting glucose (mg/dl) 90.5 93.0 0.43 • IGT 36.1% 23.2% 0.18 • Cholesterol (mg/dl) 190 174 0.008 • HDL (mg/dl) 48 48 0.49 • LDL (mg/dl) 111 99 0.04 • TG (mg/dl) 125 118 0.33 • SHBG (nmol/liter 31.7 38.5 0.04 • Total T (ng/dl) 47.5 34 <0.0001 • Free T (ng/dl) 0.19 0.12 <0.0001 Christian RC, JCEM, 2003
PCOS AND CARDIOVASCULAR DISEASE • Retrospective study of Swedish women who had ovarian • wedge resection in 1950s’: • RR for MI of 7.4 • Acta Obstet Gynecol Scand, 1992;71;599 • Death certificates from women with PCOS in the UK showed no • Increase in MI above expected number • J. Clin. Epidemiol 1998; 51;581
PCOS AND CARDIOVASCULAR DISEASE • Nurse Health Study: 82.439 women followed for 14 years. • In women with very irregular menses: • RR for CHD was 1.5 (CI 1.3-1.9) • RR for fatal MI was 1.9 (CI 1.3-2.7) • JCEM, 2002; 87;2013 Prospective controlled studies on CVD morbidity and mortality in PCOS are LACKING
Evaluation of metabolic anomalies In PCOS patients
Evaluation of Women with PCOS: Metabolic issues • Check for : • Glucose intolerance (OGTT) • Position of the Androgen Excess Society (2008) • Women with PCOS regardless of their weight should be • Screened for IGT and DMII by an OGTT at presentation • And every 2 yrs. • HTA • Dyslipidemia • Risk factors for heart disease
Traditional and novel therapy for PCOS patients
Traditional and Novel Goals of Therapy in PCOS • Improve reproductive function/fertility • Decrease risk of endometrial cancer • Treatment of acne and hirsutism • Ameliorate complications putatively due to insulin resistance • Prevent IGT and DM • Prevent ATS and acute cardiac events
PCOS: Management • Menstrual cycle irregularity/Chronic unopposed estrogen exposure: Oral contraceptives (avoid levonorgestrel) Cyclic progestin therapy • medroxyprogesterone acetate 10mg x10d every other month • Natural progesterone 200mg x 12d every month Metformin? (need for monitoring)
PCOS: Management • Hirsutism • Oral contraceptives • Oral contraceptives + antiandrogen (spironolactone) • Insulin lowering agents ineffective • Direct hair removal (laser and electrolysis) • Topical agents (eflornithine) Martin et al. JCEM 2008
PCOS: Management Infertility • Weight loss! • Ovulation induction (metformin vs clomiphene)
PCOS: Management Prevention of IGT and Type II diabetes
Prevention of type II DM in non-PCOS Population • Diabetes Prevention Program Research Group 2002 (DPP) • Large placebo controlled RCT on 3234 subjects in the US with high risk of developing DM • Gestational DM • Presence of IGT • First degree relative with DM • Subjects were randomized to • Standard management • Intensive life style intervention • Metformin • Troglitazone (discontinued after 18 M– hepatic dysfct) • DPP Group, NEJM, 2002
Prevention of DMII in non-PCOS Population (DPP) Mean F/U of 2.8 yr • Intensive life style intervention incidence of new type II DM by 58% • Metformin incidence of new type II DM by 31% Improvement in insulin sensitivity either through intensive life Style modification ++ or metformin reduces the risk of developing DM in High risk population DPP Group, NEJM, 2002
Metformin and Prevention of IGT in PCOS • Limited data on the long-term beneficial effect of Metformin on the • risk for type II DM in women with PCOS. • One retrospective study of PCOS women treated with metformin for an • average of 43 M • At baseline: 78% had NGT & 22% had IGT • At F/U: No woman developed DM • IGT group: 45% continued IGT • 55% revert to NGT • NGT group: 5% converted to IGT • 95% continued NGT • 11-fold decrease in the annual conversion rate from NGT to IGT • with 55% of IGT patients reverting to NGT Sharma et al End. Pract, 2007