Download
1 / 97
1.07k likes | 1.98k Views
Giuseppe Giaccone, MD PhD Chief, Medical Oncology Branch and Affiliated Branches. Tyrosine Kinase Inhibitors in non-small cell lung cancer. Estimated Cancer Death Rates in the United States 2009 Men 292,540; Women 269,800. Lung and bronchus 30% Prostate 9% Colon and rectum 9% Pancreas 6%

E N D
Giuseppe Giaccone, MD PhD Chief, Medical Oncology Branch and Affiliated Branches Tyrosine Kinase Inhibitors in non-small cell lung cancer
Estimated Cancer Death Rates in the United States 2009Men 292,540; Women 269,800 Lung and bronchus 30% Prostate 9% Colon and rectum 9% Pancreas 6% Leukemia 4% Liver 4% 26% Lung and bronchus 15% Breast 9% Colon and rectum 6% Pancreas 5% Ovary 4% Non-Hodgkin’s Lymphoma
Lung Cancer Demographics • Second most frequently diagnosed cancer in the United States • ~12% of all new diagnoses • ~173,770 individual cases in 2004 • Median age at diagnosis is approximately 70 years • Over 1/3 of all diagnoses are made in patients over 75 years of age • Leading cause of cancer deaths in the United States • ~160,440 patients will die in 2004 • 32% and 25% of all cancer deaths in American men and women, respectively
U.S. Cancer Mortality: Men Women
NSCLC: United States Survival Over 3 Decades. The % 5 year was:13.9% in 197515.0% in 197815.1% in 198115.5% in 198415.1% in 198715.8% in 199016.3% in 199316.9% in 1997
Lung cancer Lung cancer in never smokers:The 7th leading cause of cancer deaths in the world
Tyrosine kinases within the kinome From Cell Signaling
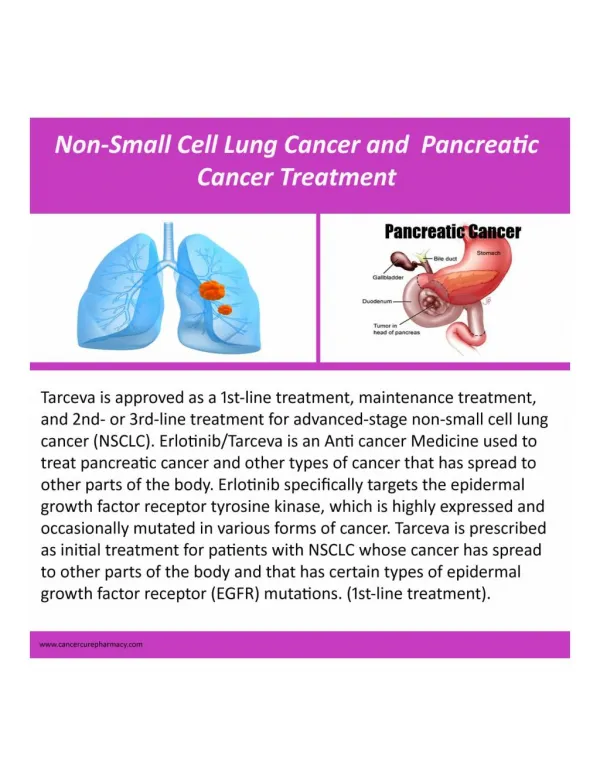
Approved molecularly targeted agents in advanced NSCLC • Erlotinib and gefitinib in patients who received prior chemotherapy • No patient selection • Gefitinib for EGFR mutants (EMEA) • Bevacizumab in first line with carbo-taxol (FDA) or with a platinum-based regimen (EMEA) • Non-squamous, no hemoptysis, no brain metastases
EGFR inhibitors in NSCLC-The EGFR tyrosine kinase inhibitors (erlotinib and gefitinib) have clinical activity in about 10% of metastatic NSCLC patients. -But no survival advantage has been obtained by the combination with standard chemotherapy-Activity has been associated with activating EGFR mutations
EGFR mutations and response to EGFR-TKI in advanced NSCLC ●Mutation frequency approximately 12% in Caucasians●More frequent in never-smokers, women, adenocarcinoma, BAC and Asians ●Rare or absent in other tumor types●Presence of a mutation predicts response to small molecules EGFR inhibitors●Presence of EGFR mutations confers distinct survival advantage (20 m vs 8 m) upon treatment with EGFR TKIs●Early event in lung carcinogenesis
H1781 H1666 H441 H3255 EGFR L858R is more sensitive to gefitinib in vitro 120 100 80 60 40 20 0 Percent control 0.001 0.01 0.1 1 10 Gefitinib concentration (µM)
BR.21: erlotinib phase III study in advanced, relapsed NSCLC • n=731 patients • Primary objective: overall survival • Secondary objectives: response rate, stable-disease rate, duration of response, time to disease progression, and QoL stage IIIB/IV, relapsed NSCLC; PS 0–3;● failed one or two prior regimens Placebo of erotinib (150 mg/day) injection
Overall SurvivalAll PatientsHR = 0.72, p = 0.001Erlotinib Median = 6.7 mo (n=488)Placebo Median = 4.7 mo (n=243) 1-yr Survival = 31%1-yr Survival = 21% 1.00 0.75 0.50 Survival Distribution Function 0.25 0.00 0 5 10 15 20 25 30 Survival Time (Months)
Tumor Response in Selected Subsets. ●The response rate is 14.4% for females and 6.0% for males (p = 0.0065).●The response rate is 13.9% for patients with adenocarcinoma and 3.8% for patients with squamous carcionoma (p = 0.0020).●The response rate is 24.7% in never smokers and 3.9% in smokers.
First line erlotinib in advanced NSCLC Response (n=53) 1 patient had a complete response lasting 183 days. 11 patients had a Partial response lasting 256 days. 17 patients had stable disease lsting 84 days. 12 patients had Progressive disease and 12 patients were Not evaluable at 6 weeks.
Correlation of smoking status and tumor type with responseIn patients who Never smoked, 3 females with adenocarcinoma had PR and 1 had SD.In females with BAC 3 had a PR. In females with other histology 2 had SD. In males with BAC 1 had PR.In former or current smokers, females with adenocarcinoma had 2 PR and 6 SD. Females with SCC and LCC each had 1 SD. Males with adenocarcinoma had 1 CR and 1SD. Males with SCC had 2 PR and 1 SD. Males with LCC or BAC had 3 and 1 SD respectively.
MO17426: mutation analysisOf 28 patients utations of the EGFR occurred in 4/5 responders, 1/12 with SD and 0/11 non-responders. Of 28 patients with PI3K mutations, 0/3 were responders, 1/11 with SD, and 0/11 nonresponders. Of patients with K-ras mutations, 0/4 responded/ 3/10 had SD and 7/11 were non-responders.
Incidence of EGFR gene mutations (global data from literature; n=2880).EGFR mutations occur in Asian females who smoke and get adenocarcinoma
IPASSPatients are Chemonaïve and Age ≥18 years. Patients should have Adenocarcinoma histology and a smoking history of Never or light ex-smokers*. The Life expectancy should be greater than 12 weeks and the tumor stage should be Measurable stage IIIB / IV disease. Patients are treated with gefitinib (250 mg/day) or carboplatin (AUC 5 or 6) with paclitaxel (200 mg/m2) 3 times weekly. Primary endpoints are Progression-free survival , whereas secondary endpoints are Objective response rate, Overall survival, Quality of life, Disease-related symptoms Safety and tolerability. Exploratory Biomarkers include EGFR mutation,EGFR-gene-copy number and EGFR protein expression.
Study conduct 87 centres in 9 countries in Asia China, Hong Kong, Indonesia, Japan, Malaysia, Philippines, Singapore, Taiwan, Thailand 1217 patients randomised Randomisation period: March 2006 to October 2007 Data cut-off: 14 April 2008 950 PFS events observed in ITT population (78% maturity) Mean time on treatment gefitinib, 6.4 months carboplatin / paclitaxel, 3.4 months (median number of cycles#: 6) Final survival data (944 events) expected mid-2010 Hong Kong Myanmar #limited to a maximum of 6 cycles PFS, progression-free survival; ITT, intent-to-treat
Demography (ITT population) % Gefitinib %Carbo/pacli- (n = 609) taxel (n= 609)Age <65 years 73 74Median age (range), years 57 57Femalea 79 79WHO PS0 / 1 / 2a 26/64/10 26/63/11Never smokera 94 94Light ex-smokera 6 6Mean smoking duration, years 11.5 14.5Mean time since cessation, years 24.6 23.4Metastatic disease 75 76Time since diagnosis: <6 months 96 94Chinese ethnicity 52 50Japaneseethnicity 19 20
Attrition rates in biomarker analysis1217 randomisedpatients (100%) 1038biomarker consent (85%) 683 provided samples (56%) Evaluable for:EGFR mutation: 437 (36%)EGFR gene copy number: 406 (33%)EGFR expression: 365 (30%)
EGFR Mutation Rate(Asian, Non-/Light Smoker, Adenocarcinoma) 59.7% (261 / 437)
Prospective Studies of Patients with EGFR mutations treated with EGFR TKIs. The relative response to gefitinib ranges from 55-82%. The time to progression ranges from 9.4 to 13.3 months.
IPASS: Objective tumour response (N=609) (N=608)
Progression-free survivalin a population with 60% EGFR mutation rate Probabilityof PFS Carboplatin / paclitaxel 1.0 Gefitinib N Events 609 453 (74.4%) 608 497 (81.7%) 0.8 HR (95% CI) = 0.741 (0.651, 0.845) p<0.0001 0.6 5.874%48%7% Median PFS (months)4 months progression-free6 months progression-free12 months progression-free 5.761%48%25% 0.4 Gefitinib demonstrated superiority relative to carboplatin / paclitaxel in terms of PFS 0.2 0.0 0 4 8 12 16 20 24 Months At risk : Gefitinib 609 363 76 24 5 0 212 Carboplatin / paclitaxel 608 412 118 22 3 1 0
IPASS: EGFR Mutation and Progression-free survival EGFR mutation positive EGFR mutation negative Gefitinib (n=132)Carboplatin / paclitaxel (n=129) Gefitinib (n=91)Carboplatin / paclitaxel (n=85) 1.0 1.0 HR (95% CI) = 0.48(0.36, 0.64) p<0.0001 No. events gefitinib, 97 (73.5%)No. events C / P, 111 (86.0%) HR (95% CI) = 2.85 (2.05, 3.98) p<0.0001 No. events gefitinib , 88 (96.7%)No. events C / P, 70 (82.4%) 0.8 0.8 0.6 0.6 Probability of progression-free survival Probability of progression-free survival 0.4 0.4 0.2 0.2 0.0 0.0 0 4 8 12 16 20 24 0 4 8 12 16 20 24 Months Months At risk : Gefitinib 132 108 31 11 3 0 91 21 2 1 0 0 71 4 C / P 129 103 37 7 2 1 0 85 58 14 1 0 0 0
Comparison of PFS by mutation status within treatment arms Gefitinib EGFR M+ (n=132)Gefitinib EGFR M- (n=91)Carboplatin / paclitaxel EGFR M+ (n=129) Carboplatin / paclitaxel EGFR M- (n=85) Probabilityof PFS 1.0 Gefitinib, HR=0.19, 95% CI 0.13, 0.26, p<0.0001No. events M+ = 97 (73.5%)No. events M- = 88 (96.7%) Carboplatin / paclitaxel, HR=0.78, 95% CI 0.57, 1.06, p=0.1103No. events M+ = 111 (86.0%)No. events M- = 70 (82.4%) 0.8 0.6 0.4 0.2 0.0 0 4 8 12 16 20 24 Time from randomisation (months)
Overall survival in ITT population (follow-up ongoing) Gefitinib Carboplatin / paclitaxel Probabilityof survival 1.0 N Events 609 223 (36.6%) 608 227 (37.3%) HR (95% CI) = 0.91 (0.76, 1.10) 0.8 Median OS (months)6 month OS12 month OS 18.684%68% 17.386%64% 0.6 0.4 0.2 0.0 0 4 8 12 16 20 24 28 Months At risk : Gefitinib 609 514 239 118 38 0 0 423 Carboplatin / paclitaxel 608 524 401 212 104 32 1 0
37/63 (59%) of pts with acquired resistance display 2nd-site EGFR mutations 94% 3% 3%
Mechanisms of Acquired ResistancePatients with acquired resistance to Gefitinib/Erlotinib●Approximately 50% have EGFR T790M mutations which can be treated with a second generation EGFR inhibitor●Approximately 50% have EGFR T790M mutations and 30 percent of those are unresponsive. 20 percent have MET amplification and can be treated with a MET inhibitor
CausesMain Type Resistant EGFR mutations acquired Met amplification acquired HER2 mutations intrinsic Other receptor kinases (e.g. IGF1R) acquired EMT acquired K-RAS mutations intrinsic Strategies Second-generation EGFR inhibitors Met inhibitors Hsp90 inhibitors EGFR Resistance EMT = epithelial-mesenchymal transition; IGF1R = insulin-like growth factor 1 receptor
Acquired EGFR mutations confer resistance to gefitinib, but not all EGFR inhibitors
PF-00299804in vitro Kinase Activity – Potent panHER TKI In vitro Kinase Assays Cellular EGFR (NIH3T3/EGFR) Cellular ERRB2 (NIH3T3/ERRB2) EGFR ERRB2 ERRB4 IC50 (nM) IC50 (nM) IC50 (nM) IC50 (nM) IC50 (nM) PF-00299804 6.0 45.7 73.7 5.8 41 gefitinib 3.1 343 476 14.4 >500 erlotinib 0.56 512 790 19.3 299
PF-00299804 in vitro Activity against EGFR, HER2 and KRASmut NSCLC Cell Lines
Mutated YFP-tagged EGFR intracellular domain activate the downstream signalsWild type and S768N cells have YFP-EGFR.L858R, N771GY and 767A-769Vdup cells have YFP-EGFR and pY1092EGFR. EGFR YFP-EGFR-ICD YFP 688 JM TK TK Reg Reg 1116 YFP signal
Quantification of phosphorylated YFP-tagged EGFR protein YFP signal Wild type AF549 signal (pEGFR expression) L858R YFP background N771GY A767-V769dup S768N AF594 signal AF594 background Antibody:pEGFR Y1092 YFP signal (EGFR expression)