Download
1 / 39
420 likes | 751 Views
GASTROENTEROLOGY 2013;145:946–953. Therapeutic Potential of Fecal Microbiota Transplantation. Dr.Mohamed Shekhani. Introduction:. GIT contains large/diverse microorganisms , bacteria most.

E N D
GASTROENTEROLOGY 2013;145:946–953 Therapeutic Potential of Fecal Microbiota Transplantation Dr.MohamedShekhani
Introduction: • GIT contains large/diverse microorganisms, bacteria most. • At least 1014 bacteria is dominated by strict anaerobes includes 1000s of different species, many not yet cultured. • These bacteria: • Interact with the intestinal mucosa. • Influence intestinal permeability • Important for the absorption, distribution, metabolism, excretion of nutrients • Trigger (auto) immunity.
Introduction: • The composition of the human intestinal microbiota is associated with human health. • The composition of the intestinal microbiota can be altered with: • Diet • Prebiotics • Probiotics • Antibiotics, which produce large changes in the bacterial composition of the intestines. • Recently with FMT.
Diet: Prebiotic effects or probiotic containing • Dietary Fiber: Nonstarch polysaccharides of plant foods poorly digested by human enzymes. • Solublecomponents: pectiin, hemicelluloses, gums,mucilages;are completely fermented by the bacterial flora • Insoluble components are cellulose, some hemicelluloses, waxes, and lignin primarily in plant cell walls as well as resistant starch are only slightly fermented • Some diet contains probiotics with positive effects on health as yogurt.
Diet fibers:benefits • 1. Slows transit in small bowel • 2. Increases stool bulk • 3. Holds on to water • 4. Forms gels • 5. Binds minerals and organic substances • 6. Stimulates bacterial growth • 7. Metabolized to SCFA
Prebiotics: • Nonstarch polysaccharide or other substance supplements poorly digested by human enzymes that that stimulate growth of bacteria: • Fructo-oligosaccharides • Inulin • Galacto-,galactosyllactose-,xylo-,isomalto-and soya oligosaccharides • Pyrodextrins (glucose oligosaccharides) • Lactulose • Breast milk oligosaccharides
Probiotics: • Human microorganisms fed as supplements that benefit the host. • Human origin • Resist upper GI tract secretions • Adhere to human intestinal cells • Colonize the human intestinal tract • Production of antimicrobial substances • Antagonize carcinogenic/ pathogenic flora • Safe in clinical use at > 1010 • Stimulate immune process • Fermentation
Probiotic Organisms in USE • Bifidobactor sp. (bifidum, longum, breve,animalis, infantis,adolescentis) • Streptoccus thermophilus • Saccharomyces boulardii,cerevisiae • Enerococcus faecium • Lactobaciilli sp. (casei, acidophilus, bulgaricus, gaseri) • L.rhamnosus, GG • Lactococcus sp. (lactis,cremaris)
CLAIMS FOR PROBIOTICS • Increase resistance to infection • Decrease duration of diarrhea disease • Stimulate immunity, modulate cytokine gene expression, stimulate phagocytosis • Beneficial effect on blood pressure,serum cholesterol, diabetes mellitus,lactose digestion and allergy • Regression of tumors and reduction in carcinogens
Antibiotics: effects on intestinal microbiota • Antibiotic –associated colitis; PMC, CDI: Clindamycin,lincomycin etc. • Treated by Vancomycin or metronidazole. • Antibiotics used as therpay through intmicrobiotal composition manipulation: neomycin,Rifazimin,metronidazole for HE. • Metronidazole: in Crohn’s disease. • Rifaximin for IBS-DP.
FMT: History • The 1st description of human donor feces as a therapeutic agent from China,5th century, Ge Hong, in the Handbook of Emergency Medicine , prescribed ingestion of feces for a variety of conditions. • Ralph Lewin“: consumption of fresh, warm camel feces has been recommended by Bedouins as a remedy for bacterial dysentery; • Its efficacy was confirmed by German soldiers in Africa during ww2” • The 1st use inmainstream medicine in 1958 for PMC/CDI by Eiseman et al. • FMT has since increased in popularity due to its efficacy/ ease of use for the treatment of CDI.
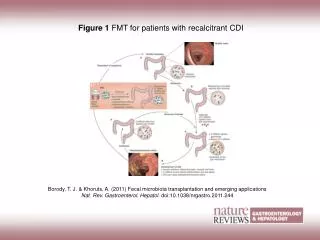
Methods of FMT: • FMT: the administration of a fecal solution from a donor into the intestinal tract of a recipient. • Donor selection. • Solution preparation. • Administration of the transplant material.
Donor selection: • Healthy donors from family members or friends ,newspaper advertisements. • Potential donors should be questioned about their travel history, sexual behavior, previous operations, blood transfusions&other factors that increase the risk of transmissible disease. • Sightly higher rate of disease resolution if from related donors. • No significant differences if different sex than the recipient. • Donor / recipient microbiota composition including enterotypes could increase the efficiency of FMT.
FMT preparation: • With Water > NS ,but higher relapse. • With milk or psyllium. • 250 ml in NS. • Freshly passed within 6 hous better, but frozen banked stool nearly similar. • Avoid electrical blender.
Route of adminstration: • Colonoscopy ,RETENTION ENEMA or OGD ,NGT,NJT. • Via colonoscopy better results.
Clinical use: • Relapsing CDI or severe CDI. • (IBD) alone or complicated by CDI • Previously unconsidered conditions
Relapsing CDI: • The antibiotic- associated R-CDI is the most common indication. • RlapsingCDI has lower proportions of Bacteroides/ Firmicutes& antibiotics such as metronidazole / vancomycin do not eradicate CDI in a large proportion of patients& fail to correct the underlying microbialdeficiencies, but FMT doesthat & cures > 90%.
Severe CDI: • FMT cures it as primary trt 84% or secondary after vanco trial 90%.
CDI in IBD: • The latest ACG guidelines recommend CDI testing of all patients hospitalized for IBD flares.
IBD: • IBD have reduced numbers of the phyla Firmicutes/ Bacteroidetes&increased numbers of Actinobacteria/ Proteobacteria . • Findings indicate that remission of UC is possible with (multiple) FMTs for a subgroup of patients. • There are currently 6 registered trials testing FMT for patients with IBD.
IBS: • Some studies: Altered intestinal microbiota (decreased diversity &numbers of Bacteroidetes ) in subsets of IBS. • There are 50 published cases of use of FMT to treat patients with diarrhea-predominant IBS & chronic constipation • Substantial improvements were reported in 30 patients (60%), who had improved defecation&anabsence of bloating and abdominal pain.
CFS: • In an uncontrolled study of 60 patients with chronic fatigue syndrome and gastrointestinal dysfunction treated with FMT, 50% had resolved sleep deprivation, lethargy, or fatigue during a 15- to 20-year follow-up period.
Metabolic/CVD: • Alterations in the composition of the intestinal microbiotahave also been associated with obesity /T2DM. • Alterations in the intestinal microbiotamight contribute to the development of cardiometabolicdiseases by increasing intestinal permeability; metabolic endotoxemia, chronic inflammation • Obese subjects have increased postprandial plasma levels of bacteria or their proteins (mainly lipopolysaccharide or endotoxin) because of increased intestinal permeability. • FMT from lean donors significantly increased insulin sensitivity, by increasing concentrations of butyrate-producing intestinal bacteria in small & large intestine. • FMT-based intervention studies are currently under way to see if can reduce features of fatty liver disease &vascular inflammation.
Adverse effects: • Safe till now. • Most patients experience diarrhea on the day of infusion. • A small %: belching/or abdominal cramping or constipation. • 3 /317 (UGIB, peritonitis, enteritis). • Fever/abdominal tenderness in 3 of 4 CD patients. • Long-term follow-up studies have found that FMT is relatively free of adverse effects.
The future: • Future research could lead to the development of specific beneficial (probiotic) microbes or inhibitors of specific microbes and/or their products that can improve human health via the intestinal microbiota.
SCQs: 1. The intestinal microbiota can be always positively affected by the following except: A.Probiotics. B.Prebiotics. C. Antibiotics. D. Fecal microbiotic transplantation. E.Diet.
SCQs: 1. The intestinal microbiota can be always positively affected by the following except: A.Probiotics. B.Prebiotics. C. Antibiotics. D. Fecal microbiotic transplantation. E.Diet.
SCQs: 2. The following antibiotics can alter intestinal microbiotal composition to have positive effects on disease course except: A.Neomycin. B.Rifaximin. C. Metronidazole. D. Vancomycin. E. Lincomycin.
SCQs: 2. The following antibiotics can alter intestinal microbiotal composition to have positive effects on disease course except: A.Neomycin. B.Rifaximin. C. Metronidazole. D. Vancomycin. E. Lincomycin.
SCQs: 3. Fecal microbiotal transplantation had proven beneficial effects in randomised controlled trials for the following conditions except: A.CDI. B. T2DM. C. Insulin resistance. D. NAFLD. E. None of the above.
SCQs: 3. Fecal microbiotal transplantation had proven beneficial effects in randomised controlled trials for the following conditions except: A.CDI. B. T2DM. C. Insulin resistance. D. NAFLD. E. None of the above.
SCQs: 4. There is a better result of fecal microbiotal transplantation if the stool was taken from: A. Male. B. Female. C. Related donor. D. Unrelated donor. E. Antibiotic-treated donor.
SCQs: 4. There is a better result of fecal microbiotal transplantation if the stool was taken from: A. Male. B. Female. C. Related donor. D. Unrelated donor. E. Antibiotic-treated donor.
SCQs: 5. The best proven indication for fecal microbiotal transplantation is: A. Relapsed or sever CDI. B.IBD . C. IBS. D. Celiac disease. E. Liver cirrhosis.
SCQs: 5. The best proven indication for fecal microbiotal transplantation is: A. Relapsed or sever CDI. B.IBD . C. IBS. D. Celiac disease. E. Liver cirrhosis.