Download
1 / 1
10 likes | 115 Views
FMRIB. Figure 2: Distribution of electrodes on standard brain. Red=responders; blue=non-responders. Figure 1: Localising electrodes. Left: example patient own scan with location of stimulated contact indicated by cross hairs. Right: Location on standard brain.

E N D
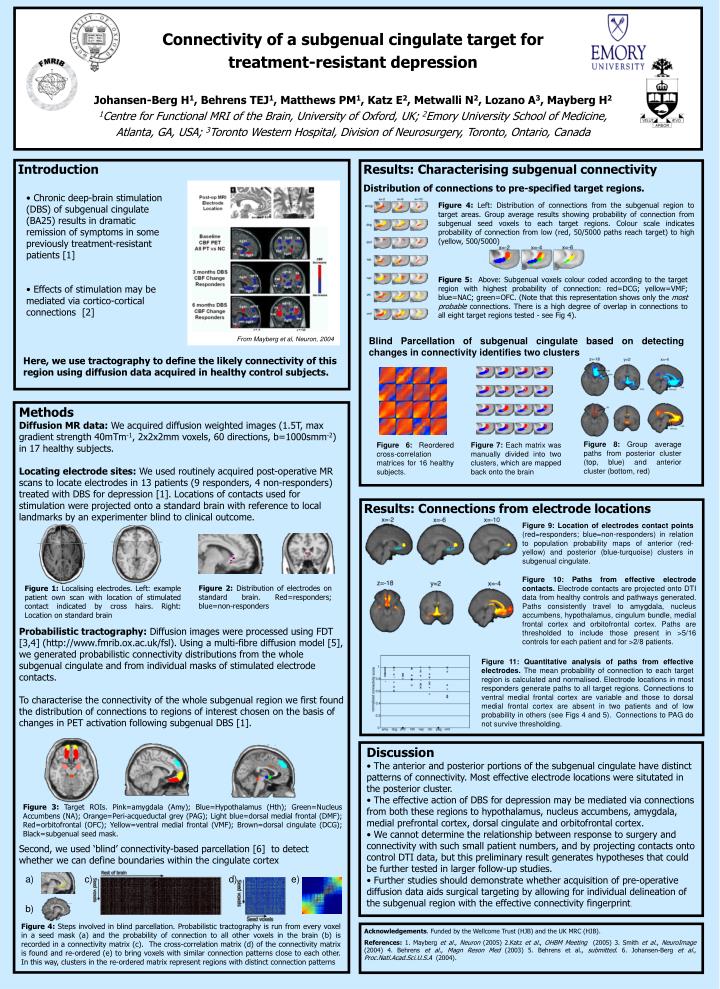
FMRIB Figure 2: Distribution of electrodes on standard brain. Red=responders; blue=non-responders Figure 1: Localising electrodes. Left: example patient own scan with location of stimulated contact indicated by cross hairs. Right: Location on standard brain Figure 3: Target ROIs. Pink=amygdala (Amy); Blue=Hypothalamus (Hth); Green=Nucleus Accumbens (NA); Orange=Peri-acqueductal grey (PAG); Light blue=dorsal medial frontal (DMF); Red=orbitofrontal (OFC); Yellow=ventral medial frontal (VMF); Brown=dorsal cingulate (DCG); Black=subgenual seed mask. a) c) d) e) b) Figure 4: Steps involved in blind parcellation. Probabilistic tractography is run from every voxel in a seed mask (a) and the probability of connection to all other voxels in the brain (b) is recorded in a connectivity matrix (c). The cross-correlation matrix (d) of the connectivity matrix is found and re-ordered (e) to bring voxels with similar connection patterns close to each other. In this way, clusters in the re-ordered matrix represent regions with distinct connection patterns Connectivity of a subgenual cingulate target for treatment-resistant depressionJohansen-Berg H1, Behrens TEJ1, Matthews PM1, Katz E2, Metwalli N2, Lozano A3, Mayberg H21Centre for Functional MRI of the Brain, University of Oxford, UK; 2Emory University School of Medicine, Atlanta, GA, USA; 3Toronto Western Hospital, Division of Neurosurgery, Toronto, Ontario, Canada Introduction Results: Characterising subgenual connectivity Distribution of connections to pre-specified target regions. • Chronic deep-brain stimulation (DBS) of subgenual cingulate (BA25) results in dramatic remission of symptoms in some previously treatment-resistant patients [1] • Effects of stimulation may be mediated via cortico-cortical connections [2] Figure 4: Left: Distribution of connections from the subgenual region to target areas. Group average results showing probability of connection from subgenual seed voxels to each target regions. Colour scale indicates probability of connection from low (red, 50/5000 paths reach target) to high (yellow, 500/5000) Figure 5: Above: Subgenual voxels colour coded according to the target region with highest probability of connection: red=DCG; yellow=VMF; blue=NAC; green=OFC. (Note that this representation shows only the most probable connections. There is a high degree of overlap in connections to all eight target regions tested - see Fig 4). Blind Parcellation of subgenual cingulate based on detecting changes in connectivity identifies two clusters From Mayberg et al, Neuron, 2004 Here, we use tractography to define the likely connectivity of this region using diffusion data acquired in healthy control subjects. Methods Diffusion MR data:We acquired diffusion weighted images (1.5T, max gradient strength 40mTm-1, 2x2x2mm voxels, 60 directions, b=1000smm-2) in 17 healthy subjects. Locating electrode sites:We used routinely acquired post-operative MR scans to locate electrodes in 13 patients (9 responders, 4 non-responders) treated with DBS for depression [1]. Locations of contacts used for stimulation were projected onto a standard brain with reference to local landmarks by an experimenter blind to clinical outcome. Probabilistic tractography:Diffusion images were processed using FDT [3,4] (http://www.fmrib.ox.ac.uk/fsl). Using a multi-fibre diffusion model [5], we generated probabilistic connectivity distributions from the whole subgenual cingulate and from individual masks of stimulated electrode contacts. To characterise the connectivity of the whole subgenual region we first found the distribution of connections to regions of interest chosen on the basis of changes in PET activation following subgenual DBS [1]. Second, we used ‘blind’ connectivity-based parcellation [6] to detect whether we can define boundaries within the cingulate cortex Figure 8: Group average paths from posterior cluster (top, blue) and anterior cluster (bottom, red) Figure 6: Reordered cross-correlation matrices for 16 healthy subjects. Figure 7: Each matrix was manually divided into two clusters, which are mapped back onto the brain Results: Connections from electrode locations Figure 9: Location of electrodes contact points (red=responders; blue=non-responders) in relation to population probability maps of anterior (red-yellow) and posterior (blue-turquoise) clusters in subgenual cingulate. Figure 10: Paths from effective electrode contacts. Electrode contacts are projected onto DTI data from healthy controls and pathways generated. Paths consistently travel to amygdala, nucleus accumbens, hypothalamus, cingulum bundle, medial frontal cortex and orbitofrontal cortex. Paths are thresholded to include those present in >5/16 controls for each patient and for >2/8 patients. Figure 11: Quantitative analysis of paths from effective electrodes. The mean probability of connection to each target region is calculated and normalised. Electrode locations in most responders generate paths to all target regions. Connections to ventral medial frontal cortex are variable and those to dorsal medial frontal cortex are absent in two patients and of low probability in others (see Figs 4 and 5). Connections to PAG do not survive thresholding. • Discussion • The anterior and posterior portions of the subgenual cingulate have distinct patterns of connectivity. Most effective electrode locations were situtated in the posterior cluster. • The effective action of DBS for depression may be mediated via connections from both these regions to hypothalamus, nucleus accumbens, amygdala, medial prefrontal cortex, dorsal cingulate and orbitofrontal cortex. • We cannot determine the relationship between response to surgery and connectivity with such small patient numbers, and by projecting contacts onto control DTI data, but this preliminary result generates hypotheses that could be further tested in larger follow-up studies. • Further studies should demonstrate whether acquisition of pre-operative diffusion data aids surgical targeting by allowing for individual delineation of the subgenual region with the effective connectivity fingerprint. Acknowledgements. Funded by the Wellcome Trust (HJB) and the UK MRC (HJB). References: 1. Mayberg et al., Neuron (2005) 2.Katz et al., OHBM Meeting (2005) 3. Smith et al., NeuroImage (2004) 4. Behrens et al., Magn Reson Med (2003) 5. Behrens et al., submitted. 6. Johansen-Berg et al., Proc.Natl.Acad.Sci.U.S.A (2004).






