Download
1 / 29
290 likes | 306 Views
Explore the historical phases of hospital development, terminology, expansion, and downsizing. Learn about nonprofit hospitals, management, and ethical issues shaping the healthcare landscape. Analyze the organizational changes and ethical challenges faced by hospitals over time, from their primitive origins to the complexities of modern healthcare systems. Identify the key drivers of hospital transformation and anticipate future trends in the industry.

E N D
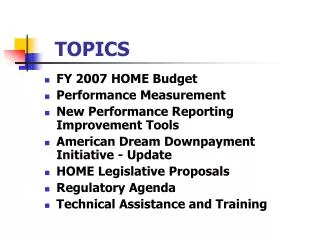
Topics • Terminology • History of Hospitals • Hospital Expansion Phases • Hospital Downsizing Phase • Hospital Organization • Nonprofit Hospitals • Hospital Management • Ethical and Legal Issues “It may seem a strange principle to enunciate as the very first requirement in a hospital that it should do the sick no harm” Florence Nightingale
Terminology • “Inpatient” involves an overnight stay at a healthcare facility • “Outpatient” does not • Usage is not dependent on the • Severity of the condition • Complexity of the treatment
Terminology (cont.) • “Hospital” • At least six beds (why not five?) • Organized physician staff • Licensed • Continuous nursing services • On site pharmacy services • Governing body and chief executive • Food service • Medical records services Which of these characteristics does a nursing home lack?
History of Hospitals • Book identifies five distinct phases • Primitive institutions of social welfare • Distinct institutions for care of the sick • Organized institutions of medical practice • Advanced institutions of medical training and research • Consolidated systems of health services delivery • We are interested in the drivers of transformation between stages • Help identify future trends
History of Hospitals (cont.) • Primitive Institutions of Social Welfare • Through the late 1800s • “Poorhouses” for the destitute • Little medical treatment • “Pesthouses” isolated the sick with contagious diseases • Very few of these institutions • Restricted to a few urban areas
History of Hospitals (cont.) • Distinct Institutions to Care for the Sick • Became widespread in the late 1800s • A few notable exceptions prior to this time • Differentiated from the Poorhouses and Pesthouses • Medical care was provided • A treatable illness was expected • Why did we see such low prominence for hospitals in the HC system? • Or, where was healthcare coming from?
History of Hospitals (cont.) • Organized Institutions for Medical Practice • Late 1800s/Early 1900s saw huge transformations in the practice of medicine • What were they? • Hint: Contrast with medical effectiveness in the past • How did they affect hospitals? • Hospitals became centers of medical practice • Why? (This is hugely important)
History of Hospitals (cont.) • Organized Institutions for Medical Practice (cont.) • Hospitals required professional management and organization • Departmental organization became common (why?) • Management had to focus on efficiency • Hospitals shifted focus to the acute stage of an illness • Early cost containment strategy
History of Hospitals (cont.) • Medical Teaching and Research • Shift in medical care to hospitals resulted in • Shift in medical education to hospital-centered knowledge • Tight coupling between (some) hospitals and medical schools • Partnerships • Unified ownership • Hospital practice for internships and residencies
History of Hospitals (cont.) • Consolidated HC Delivery Systems • Late 20th Century changes have lead to new models for hospitals • Economic pressures • Technological advances • Cost pressures and technologies have reduced hospital stays • Excess bed capacity → consolidation • Competition from new providers • Outpatient surgery centers • Imaging centers More Coming Up
Hospital Expansion Phase • Hospitals expanded exponentially from late 1800s through mid 1980s • Six drivers of expansion • Advances in medical science • Development of specialized technology • Advances in medical education • Development of professional nursing • Increased health insurance • Government involvement • Construction • Medicare and Medicaid
Hospital Downsizing Phase (cont.) • Pressures on Hospitals • Increased cost controls → Decreased reimbursement • Shorter stays • Fewer admissions • Increased competition • Improved technologies made more procedures outpatient
Hospital Downsizing Phase (cont.) • Downsizing affected hospitals in two ways • Hospital closings • Marginal hospitals failed • Smaller hospitals hard hit • Rural hospitals hard hit • Hospital mergers and acquisitions • Smaller and non-profit hospitals absorbed by larger chains • Chains seeking to increase capacity in advance of the baby book entering old age
Hospital Downsizing Phase (cont.) • What are the implications of these figures?
Hospital Organization • Hospitals come in a wide variety of • Ownership models • Services offered • Multi-hospitalstructure
Hospital Organization (cont.) • Public Hospitals • Government owned and operated • Federal ownership exclusively for special populations • State, county, & municipal focused on service to public • High proportion of lower income and uninsured • Financial and economic pressures squeezing these institutions • Community Hospital—open to all comers
Hospital Organization (cont.) • Hospital Chains • See staffing differences between independent and chain hospitals (Table 8-3) • Hospital chains realize economies of scope and scale • Administrative overhead • Billing and reimbursement • Facilities management • Governance • Information technology investments • Lengthen the value chain
Hospital Organization (cont.) • Types of Hospitals • General hospitals • Most common • Provide wide range of services • Specialty hospitals • Rehabilitation • Focused disease (cardiac, cancer) • Psychiatric • Children’s or Women’s and Children’s
Hospital Organization (cont.) • Rural vs. Urban Hospitals • Urban (county population > 100,000) • Higher costs • Broader scope of services • Rural • Disproportionate number of poor • Cannot employ many specialist staff and facilities full time • Funding increases available if designated a Critical Access Hospital
Hospital Organization (cont.) • Operational costs by size
Hospital Organization (cont.) • Teaching Hospitals • Offer residency programs • Receive targeted Medicare funding • Associated with a medical school (“Academic Medical Center”) • Training • Research • Tertiary care in one or more specialties
Nonprofit Hospitals • 80% of all private hospitals and 84% of all private hospital beds are nonprofit • Legal definition of nonprofit must be clearly understood • Research discloses little difference in the behavior between for-profit and nonprofit hospitals of similar size and location • Nonprofit hospitals receive significant tax benefits • Under review to justify these exemptions
Hospital Management • Hospitals are complex organizations • (But not the most complex) • Multiple stakeholders (List these groups!!) • Parallel governance structures distinctive • Administrative management • Medical staff • Objectives often at odds with each other • Some staff accountable to both authority chains • Pharmacy ‒ Nursing • Lab ‒ etc.
Hospital Management (cont.) • Hospitals require licensure, accreditation, and various other certifications • Affect ability to operate • Affect ability to provide reimbursable services • Hospital management must continuously monitor criteria for certifications, etc.
Ethical and Legal Issues • Healthcare is fraught with opportunities for unethical behavior regardless of motivation • Fraud and many other acts are clearly wrong • But HC providers have ethical duties to respect patient wishes even… • …if patient does not understand the science • …patient over- or undervalues a treatment • …patient does not understand the risk • Patients (or surrogate) must give consent for treatment
Ethical and Legal Issues (cont.) • Many practical ethical issues in HC revolve around “informed consent” • Patient understands the treatment and risks • Patient elects the treatment • Patients are not always able to make informed consent • Minor children • Medically incompetent • Advanced Directives can direct care in the event patient cannot